Mental health
Community mental health care services
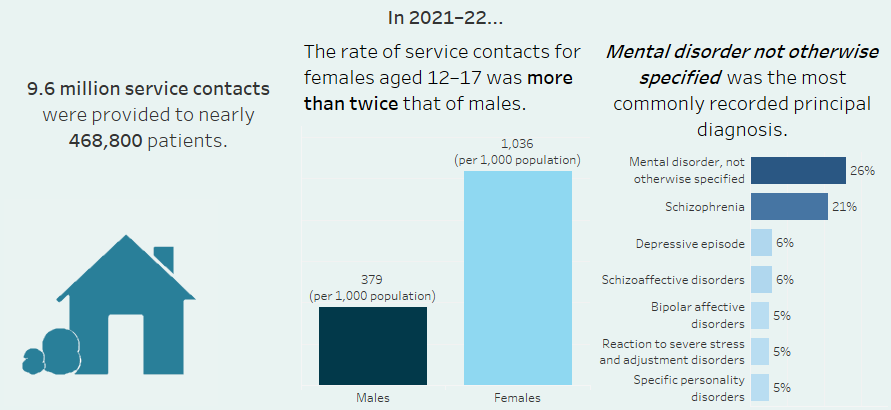
Infographic containing 3 key points from this page. An estimated 9.6 million service contacts were provided to nearly 468,800 patients in 2021-22. Mental disorder not otherwise specified (26%) was the most frequently recorded principal diagnosis, followed by Schizophrenia (21%) and the rate of service contacts was higher for females aged 12-17 than males.
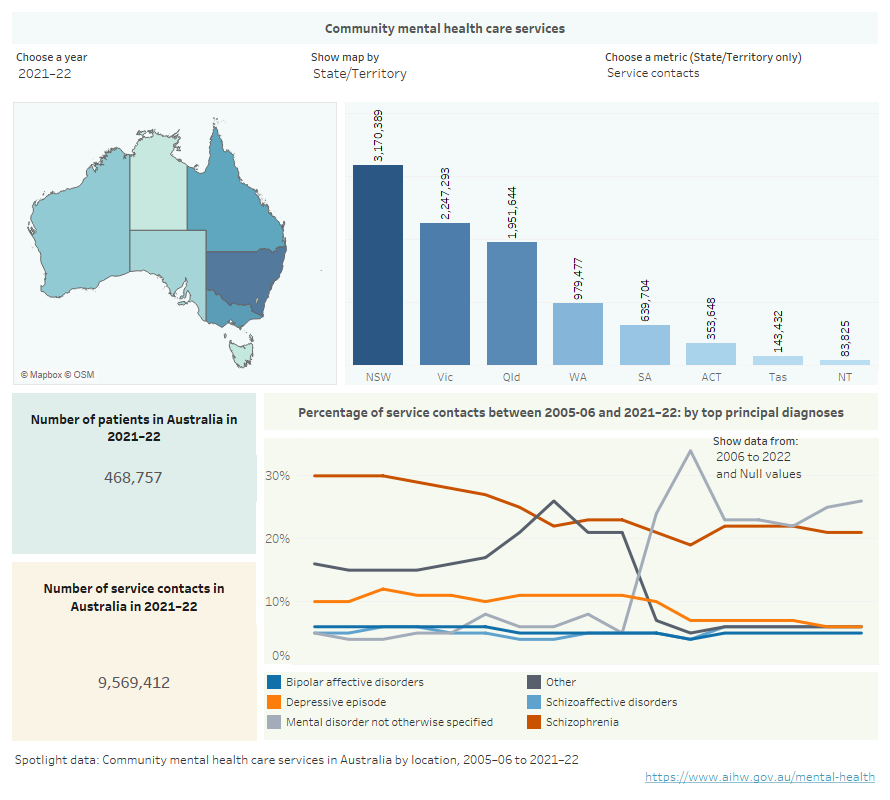
Infographic containing a map of Australia showing community mental health services by location, estimated number of patients, and principal diagnosis in community mental health care in Australia for the years 2005–06 to 2020–21.
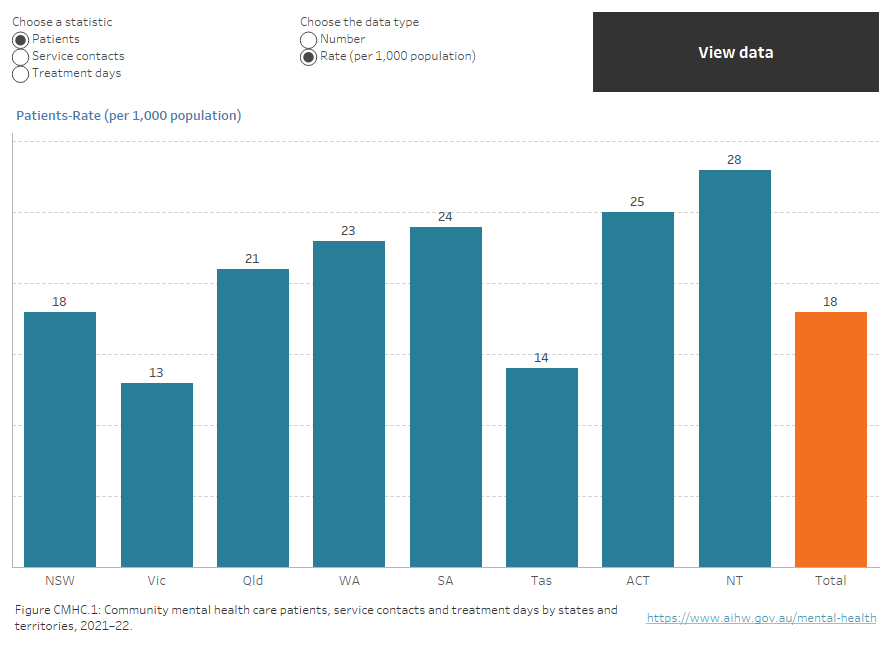
Interactive vertical bar chart showing the number of community mental health care patients, service contacts and treatment days as well as the rate of contacts and patients (rate per 1,000 population) for states and territories in 2021–22. New South Wales had the highest number of patients (142,642), followed by Queensland (108,872), Victoria (84,831), Western Australia (63,451), South Australia (42,945), the Australian Capital Territory (11,220), Tasmania (7,866) and the Northern Territory (6,930). The Northern Territory reported the highest rate (28 patients per 1,000 population) followed by the Australian Capital Territory (25), South Australia (24), Western Australia (23), Queensland (21), New South Wales (18), Tasmania (14), and Victoria (13). The national rate of community mental health care patients was 18 per 1,000 population (refer to Table CMHC.1).
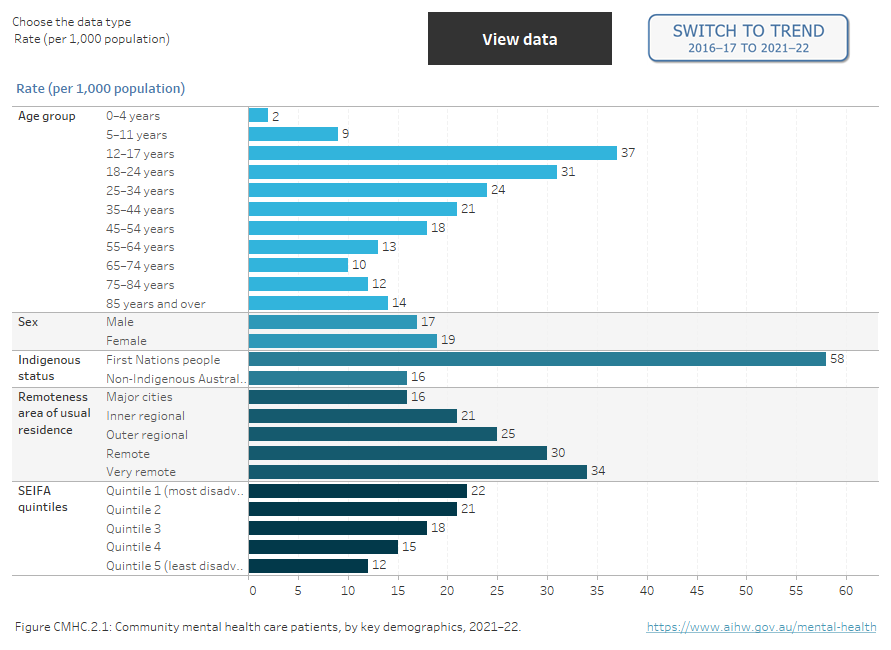
Two interactive charts. A horizontal bar chart showing the rate (per 1,000 population), per cent or number of community mental health care patients by demographic variables of age, sex, First Nations status, SEIFA quintile and remoteness area in 2021–22. The lowest rate for patients by age was seen for those aged 0–4 years (2 people per 1,000 age specific population) and the highest rate was for patients aged 12–17 years (37). Male and female patients had similar rates per 1,000 population (17 and 19 respectively). The highest rate of patients per 1,000 population by remoteness area was seen for patients living in Very remote areas (34), followed by Remote (30), Outer regional (25), Inner regional (21), and lowest for Major cities (16). The rate of patients per 1,000 population living in SEIFA Quintile 1 (most disadvantaged) was the highest of all quintiles (22), which decreased to 12 for Quintile 5 (least disadvantaged) (refer to Table CMHC.8). Figure 2 is a time series of community service contacts by patient demographics from 2005–06 to 2021–22 (refer to Table CMHC.7).
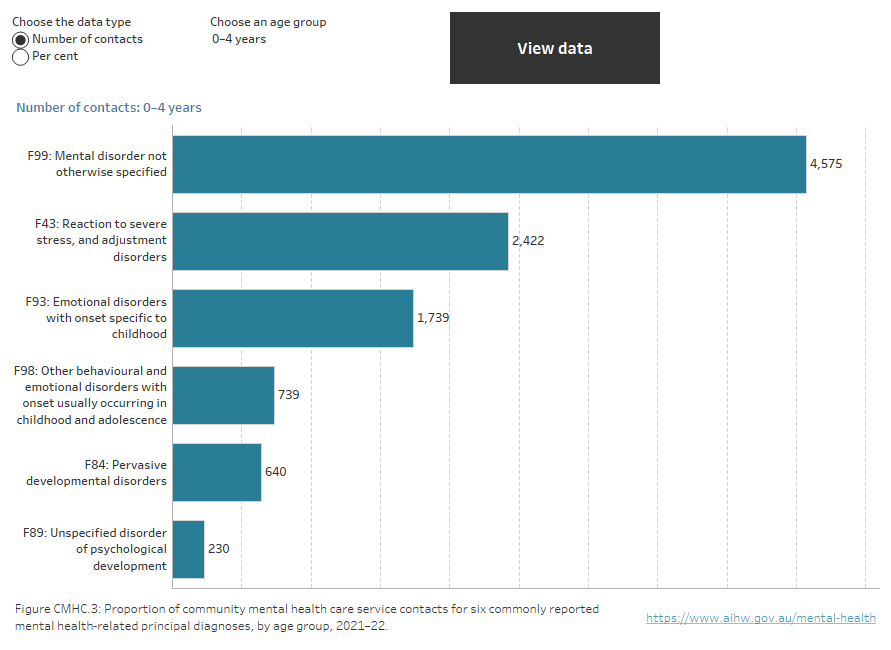
Interactive horizontal bar chart showing 6 commonly reported specific principal diagnosis for community mental health care service contacts in 2021–22 by age group. The most frequently reported principal diagnosis for those aged 0–4 years, 5–11, 12–17, 18–24, 25–34, 65–74, 75–84 and 85 and over was Mental disorder not otherwise specified (26%, 29%, 27%, 28%, 28%, 23%, 23% and 26% respectively). For older ages, Schizophrenia was the most frequently reported principal diagnosis, ranging from 29% for those aged 55–64 to 32% for those aged 45–54 years.
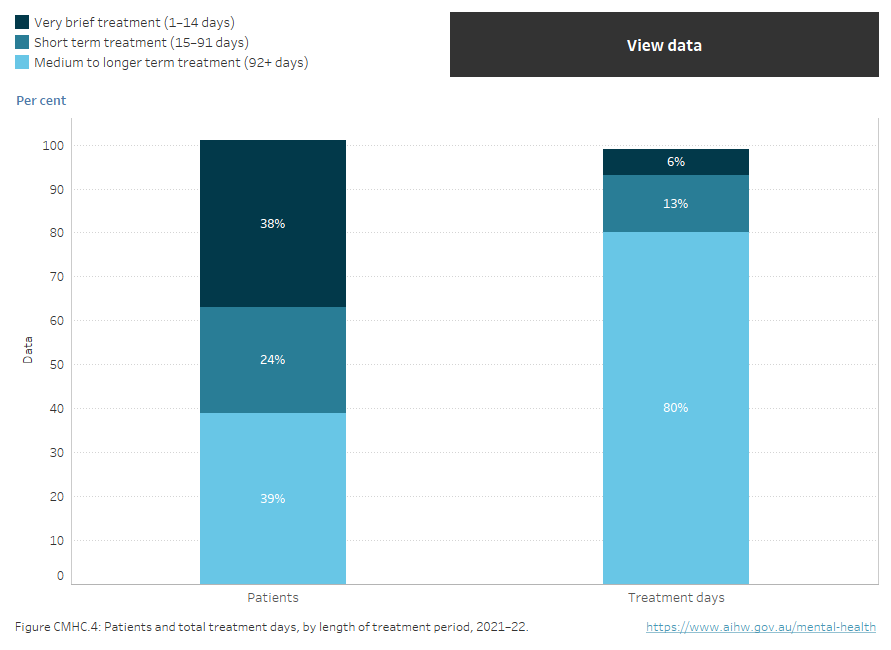
Stacked vertical bar chart showing length of treatment period and the proportion of patients that received different lengths of treatment. 38% of patients received very brief treatment (1–14 days), 24% received short term treatment (15–91 days) and 39% received medium to longer term treatment (92+ days). 6% reported treatment days were very brief, 13% were short term treatment and 80% were medium to longer term treatment (refer to table CMHC.24).
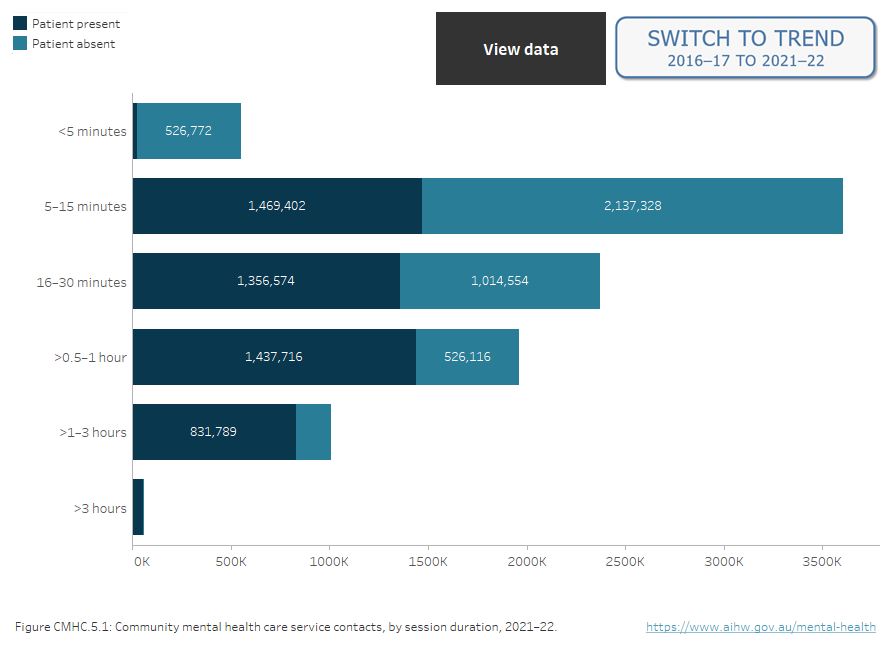
Two interactive charts. A stacked horizontal bar chart showing the duration of community mental health care service contacts by session duration and patient participation status in 2021–22. The most frequent contact duration was 5–15 minutes (38%), followed by 16–30 minutes (25%), >0.5–1 hour (21%), >1–3 hours (11%), <5 minutes (6%), and >3 hours (1%). 54% of contacts occurred with the patient present (5.2 million) and 46% occurred with the patient absent (4.4 million). Contacts lasting more than 3 hours were more likely to occur with the patient present than without the patient (1% and 0.2% respectively), while contacts lasting less than 5 minutes were more likely to occur without the patient than with the patient (12% and 1% respectively) (refer to Table CMHC.21). Figure 2 is a time series of service contacts by session duration from 2005–06 to 2021–22 (refer to Table CMHC.23).
Figure CMHC 5.2, time series of service contacts by session duration can be found on the Mental health site.