Mental health
Residential mental health care services

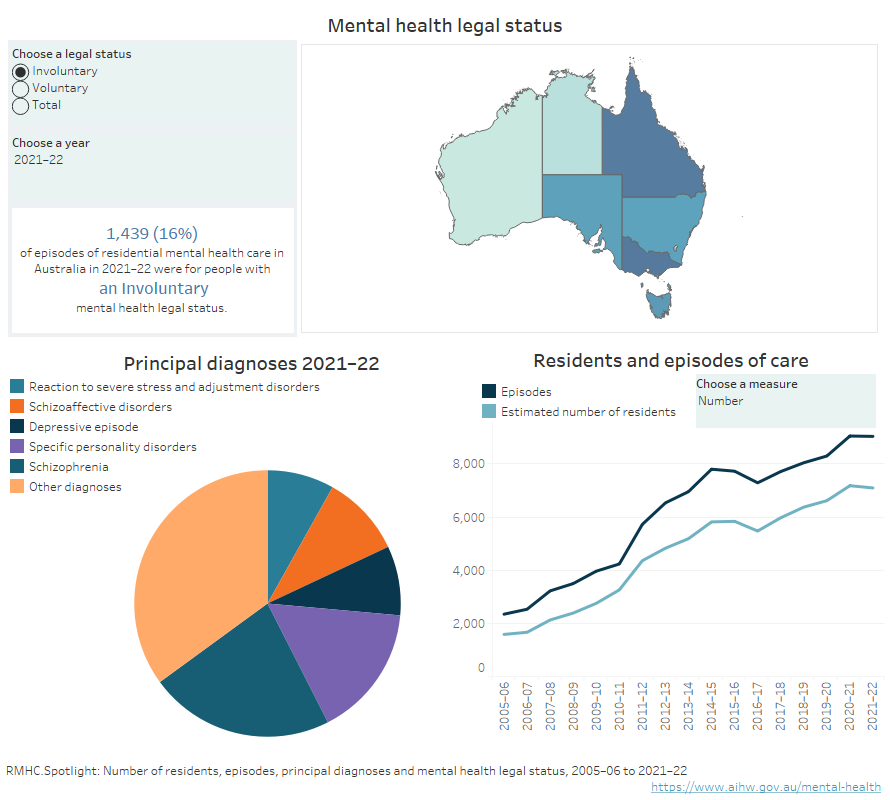
Infographic containing a pie chart showing proportions of 6 principal diagnosis categories 2021–22; a bar graph showing access by age group 2021–22; and a line chart showing the number and rate per 10,0000 population of residents and episodes of care from 2005–06 to 2021–22, (refer to Table RMHC.2 and Table RMHC.15).
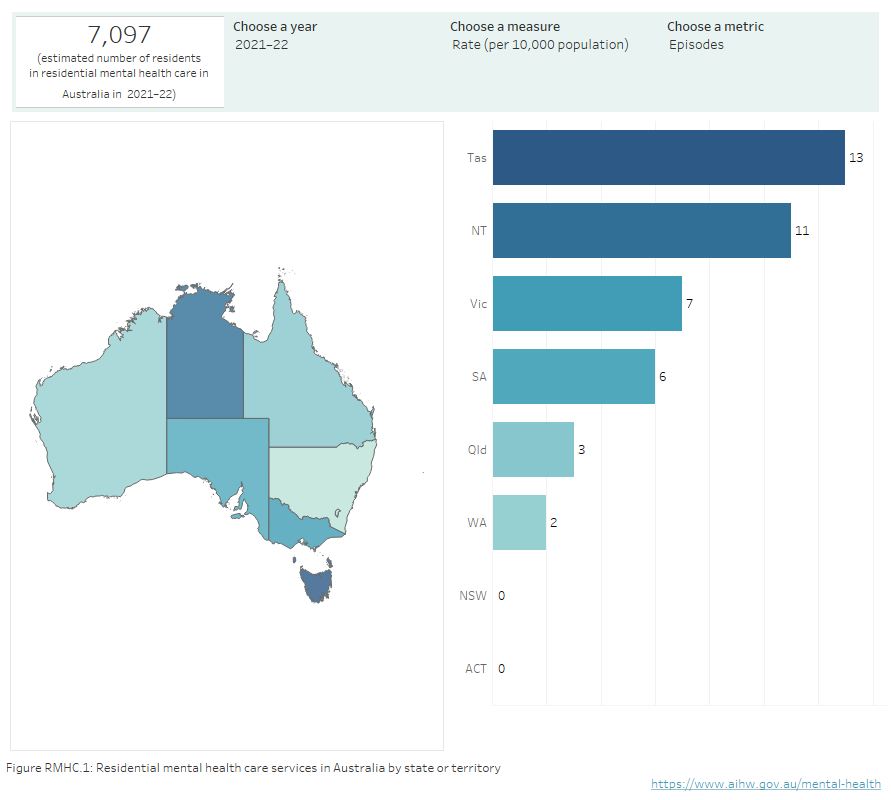
Infographic containing a map of Australia showing residential mental health care episodes, estimated number of residents and residential care days (rate per 10,000 population and number), by state or territory.
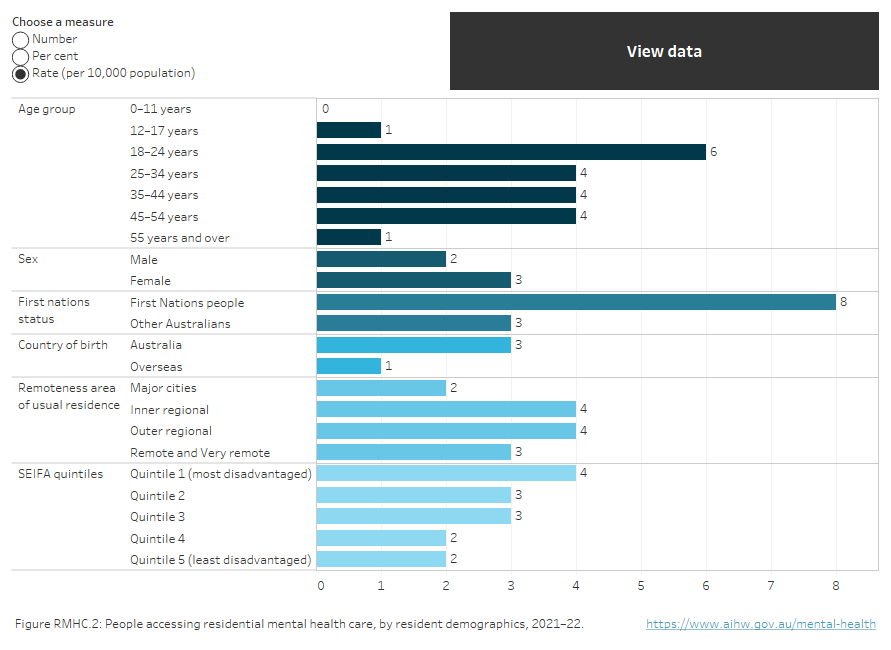
Horizontal bar chart showing the rate (per 10,000 population), per cent or number of people accessing residential mental health care by demographic variables of age group, sex, First Nations status, country of birth, remoteness area and SEIFA quintile in 2021–22. Those aged 18-24 years had the highest rate at 6. There were no residents aged under 12 years. 2 males and 3 females per 10,000 population received residential mental health care services. 8 First Nations people per 10,000 population and 3 non-Indigenous Australians received residential mental health care services. 3 people per 10,000 population who were born in Australia and 1 people who were born overseas, received residential mental health care services. The highest rates for area of usual residence were Inner regional and Outer regional at 4 people per 10,000 population, while those in Major cities had the lowest rate of 2 people per 10,000 population. SEIFA Quintile 1 (most disadvantaged) had the highest rate of people receiving residential mental health care services at 4 per 10,000 population, while Quintiles 4 and 5 had the lowest at 2 (refer to Table RMHC.3).
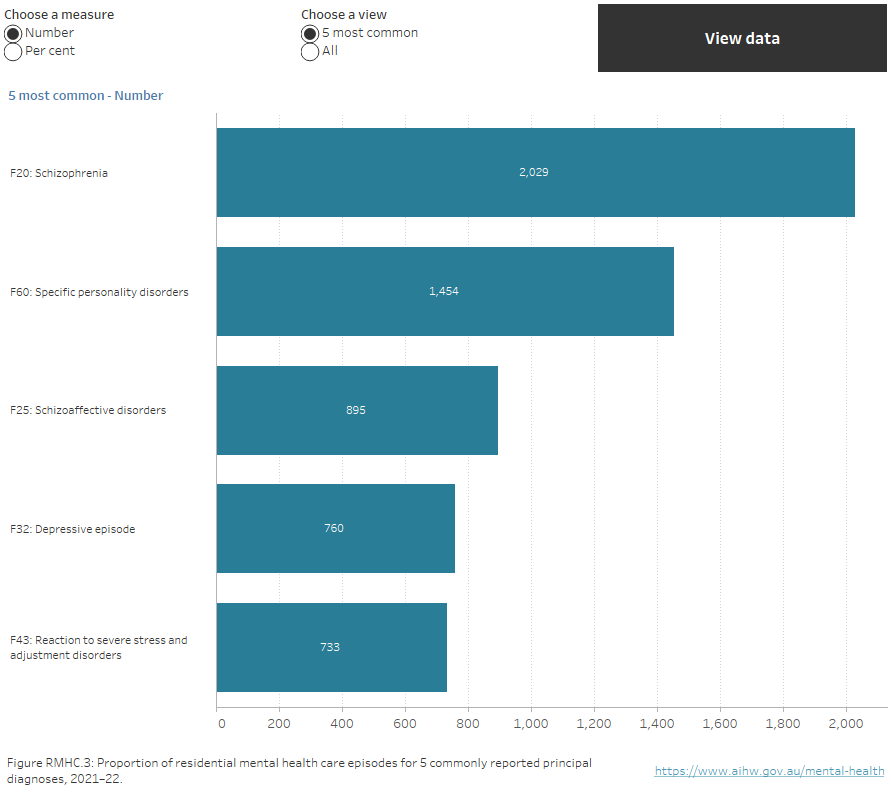
A horizontal bar chart showing the number of residential mental health care episodes with all principal diagnoses in 2021–22. Schizophrenia was recorded for 2,029 of residential mental health care episodes; Specific personality disorders, 1,454; Schizoaffective disorders, 895; Depressive episode, 760; and Reaction to severe stress and adjustment disorders, 733 (refer to Table RMHC.15).
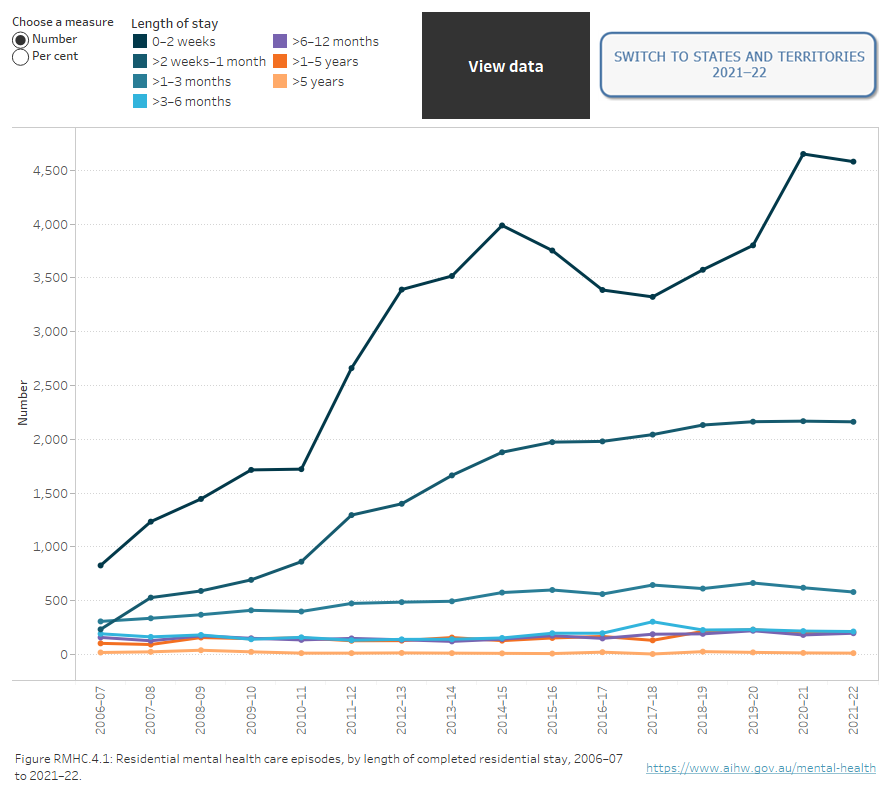
An interactive line chart showing the number of residential mental health care episodes by length of completed residential stay from 2006–07 to 2020–21. In 2020–21, episodes lasting between 0 to 2 weeks comprised 58% of episodes; between 2 weeks to 1 month, 27%; between 1 and 3 months, 7%; between 3 and 6 months, 3%; between 6 and 12 months, 2%; between 1 and 5 years, 3%; more than 5 years, 0% (refer to Table RMHC.9).