Summary
The disease burden due to risk factors is known as attributable burden. It is the amount by which disease burden would be reduced if exposure to the risk factor had been avoided or reduced to the lowest possible level. Deaths can also be attributed to risk factors using the same methods.
The Australian Burden of Disease Study 2018: Impact and causes of illness and death in Aboriginal and Torres Strait Islander people, published in 2022, estimated the disease burden and deaths due to 39 risk factor components or exposures (such as cannabis use) that combine into 19 individual risk factors (such as illicit drug use). The risk factors are categorised into 4 groups: behavioural, dietary, metabolic/biomedical and environmental. Risk factors included in this interactive web report are listed below.
This interactive report provides dynamic data displays of attributable burden and attributable deaths among Aboriginal and Torres Strait Islander people in Australia as part of the Australian Burden of Disease Study 2018.
The available estimates for Indigenous Australians include:
- Non-fatal, fatal and total attributable burden estimates by age, sex and linked disease for 2018, and for most risk factors for 2003 and 2011
- Attributable deaths estimates by sex for 2003, 2011 and 2018
- Estimates of the gap in attributable burden and deaths between Indigenous and non-Indigenous Australians for 2003, 2011 and 2018.
Risk factor estimates for a particular disease cannot simply be added together as they are estimated independently, with some risk factors being on the same causal pathway. For example, physical inactivity and high blood plasma glucose are both risk factors for coronary heart disease, but physical inactivity increases the risk of high blood plasma glucose. The ‘joint effect’ estimate is calculated in a way that takes the inter-relationships between risk factors into account. Further information on estimating attributable burden and the data and methods used in the Australian Burden of Disease Study 2018 can be found in the Australian Burden of Disease Study 2018: methods and supplementary material report. Further information on how to interpret specific measures in the visualisations is shown when hovering over the information icons on available pages.
Data visualisations displaying estimates of disease burden are available in the interactive web report: Interactive data on disease burden.
Risk factors included in the Australian Burden of Disease Study 2018: Impact and causes of illness and death in Aboriginal and Torres Strait Islander people
Behavioural risks
- Alcohol use
- Child abuse & neglect
- Illicit drug use
- Opioid use
- Amphetamine use
- Cocaine use
- Cannabis use
- Other illicit drug use
- Unsafe injecting practices
- Intimate partner violence
- Physical inactivity
- Tobacco use
- Unsafe sex
Metabolic/Biomedical risks
- Diet high in processed meat
- Diet high in red meat
- Diet high in sodium
- Diet high in sugar sweetened beverages
- Diet low in fish & seafood
- Diet low in fruit
- Diet low in legumes
- Diet low in milk
- Diet low in nuts and seeds
- Diet low in polyunsaturated fat
- Diet low in vegetables
- Diet low in whole grains & high fibre cereals
Environmental risks
- Air pollution
- Occupational exposures & hazards
- Unsafe sanitation
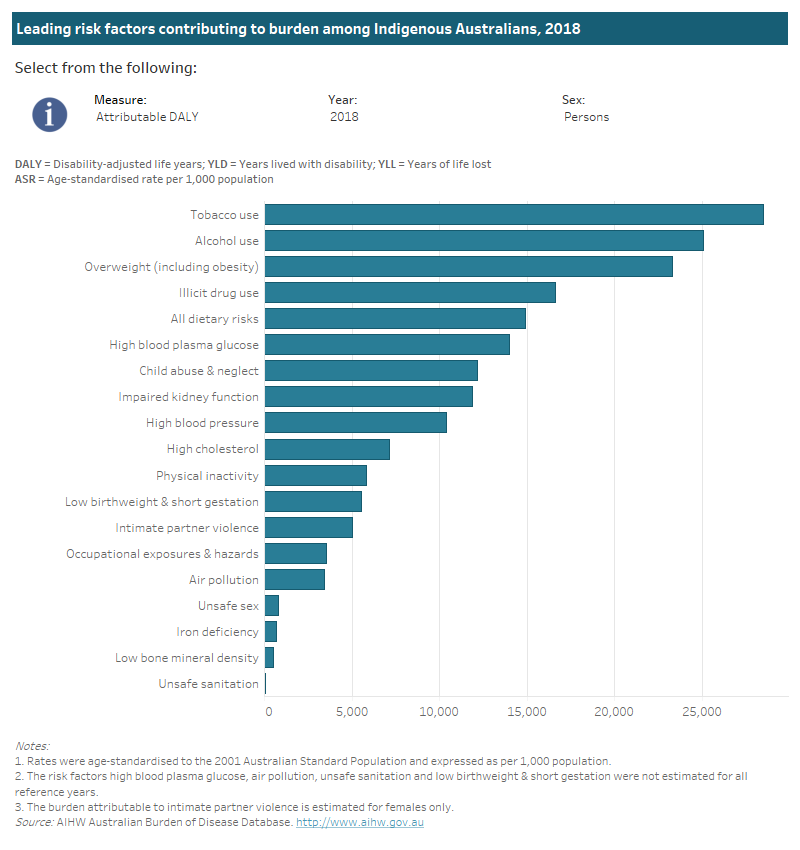
Leading risk factors
Around 49% of the burden of disease among Indigenous Australians in 2018 could have been prevented by reducing exposure to all the modifiable risk factors included in the Australian Burden of Disease Study 2018 (19 risk factors examined). This estimate has taken into account the complex pathways and interactions between diseases and risk factors.
The leading five risk factors contributing to total burden among Indigenous Australians were: tobacco use, alcohol use, overweight (including obesity), illicit drug use and dietary risks.
Tobacco use contributed the greatest amount of fatal burden and deaths among Indigenous Australians, while alcohol use contributed the most non-fatal burden.
This interactive data visualisation shows the leading risk factors by attributable burden among Indigenous Australians. The main section shows a horizontal bar graph which can be customised to report data according to sex, year and measure of attributable burden.
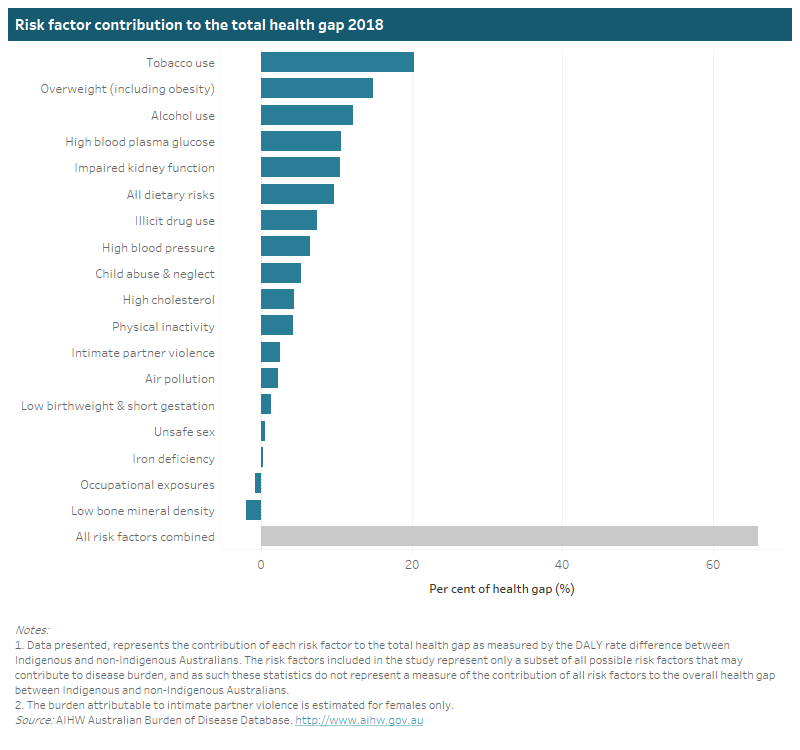
Health gap by risk factors
After adjustment for the joint effect of multiple risk factors, Indigenous Australians experienced rates of burden attributable to the risk factors included in the study at 3.5 times the rate of non-Indigenous Australians in 2018.
The leading five risk factors contributing to the gap between Indigenous and non-Indigenous populations were: tobacco use, overweight including obesity, alcohol use, high blood plasma glucose and impaired kidney function.
This interactive data visualisation shows a horizontal bar graph which presents the contribution of each risk factor to the total health gap between Indigenous and non-Indigenous Australiansin 2018.
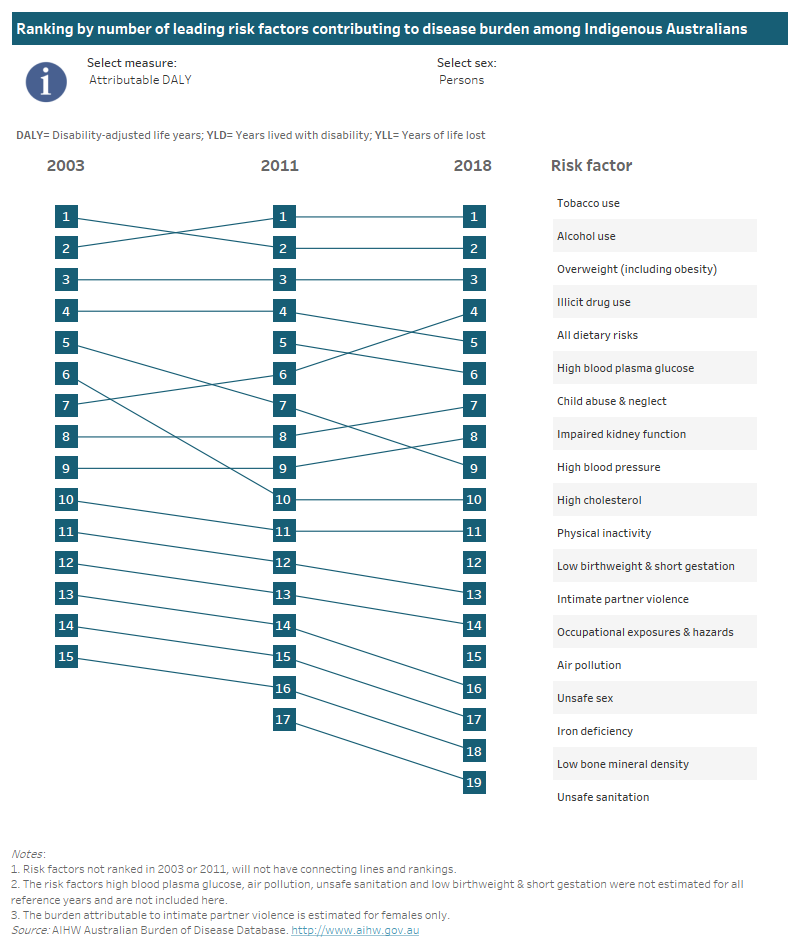
Changes in leading risk factors over time
Comparisons of attributable burden over time are provided only for those risk factors that were included in both the 2003 and 2018 estimates for Indigenous Australians. The risk factors not measured for 2003 were air pollution, high blood plasma glucose, unsafe sanitation, and low birthweight & short gestation.
It is important to consider differences between the 2003 and 2018 population size and structure when interpreting changes in burden attributable to risk factors over time. This is taken into account by looking at age-standardised rates (ASR) of burden.
Risk factors measured in both 2003 and 2018 contributed 41% of the total burden (number of DALY) among Indigenous Australians in 2003 compared with 45% in 2018, indicating an increase in the proportion of burden attributable to these risk factors. However, there are differences when looking at individual risk factors over time.
Tobacco use, overweight (including obesity), alcohol use and dietary risks were among the leading 5 risk factors for Indigenous Australians in both 2003 and 2018. High blood pressure decreased from the 5th greatest contributor to attributable burden in 2003 to 9th in 2018, while illicit drug use increased from 7th highest in 2003 to 4th highest in 2018.
Alcohol use caused the most burden of the risk factors examined in 2003, responsible for 10.4% of the total burden, and was responsible for 10.5% of the total burden in 2018. However, the contribution of alcohol use fell to 2nd as the burden attributable to tobacco use increased. The burden attributable to tobacco use rose from 10% in 2003 to 11.9% in 2018, largely the result of increased numbers of deaths from cancers related to tobacco use (linked cancers).
When looking at non-fatal burden (number of YLD), alcohol use, overweight (including obesity), child abuse & neglect, tobacco use and illicit drug use were the leading 5 risk factors among Indigenous Australians in both 2003 and 2018. Child abuse & neglect ranked 2nd in 2003 and 3rd in 2018, while overweight ranked 3rd in 2003 and 2nd in 2018.
When looking at the fatal burden (number of YLL) attributable to risk factors, tobacco use, overweight (including obesity), alcohol use and dietary risks were among the leading 5 risk factors in both 2003 and 2018. High blood pressure ranked 5th in 2003 and 7th in 2018, while illicit drug use ranked 9th in 2003 and 5th in 2018.
In terms of age-standardised rates of burden attributable to risk factors, there was a decrease of 10% between 2003 and 2018 in the joint effect of risk factors measured at both points. The rates for most individual risk factors also decreased over time, with the exception of alcohol use (which was stable at around 37 DALY per 1,000 people) and illicit drug use (which increased from 13 to 23 DALY per 1,000 people).
Tab 1: This interactive data visualisation shows the ranking of risk factors by amount of attributable burden among Indigenous Australians. The main section shows these rankings by year which can be customised to report data according to sex and measure of attributable burden.
Tab 2: This interactive data visualisation shows the ranking of risk factors by rate of attributable burden among Indigenous Australians. The main section shows these rankings by year which can be customised to report data according to sex and measure of attributable burden.