Chronic musculoskeletal conditions :
Rheumatoid arthritis
Web article
Last updated:
Citation
AIHW
Australian Institute of Health and Welfare (2023) Rheumatoid arthritis, AIHW, Australian Government, accessed 19 April 2024.
APA
Australian Institute of Health and Welfare. (2023). Rheumatoid arthritis. Retrieved from https://pp.aihw.gov.au/reports/chronic-musculoskeletal-conditions/rheumatoid-arthritis
MLA
Rheumatoid arthritis. Australian Institute of Health and Welfare, 14 December 2023, https://pp.aihw.gov.au/reports/chronic-musculoskeletal-conditions/rheumatoid-arthritis
Vancouver
Australian Institute of Health and Welfare. Rheumatoid arthritis [Internet]. Canberra: Australian Institute of Health and Welfare, 2023 [cited 2024 Apr. 19]. Available from: https://pp.aihw.gov.au/reports/chronic-musculoskeletal-conditions/rheumatoid-arthritis
Harvard
Australian Institute of Health and Welfare (AIHW) 2023, Rheumatoid arthritis, viewed 19 April 2024, https://pp.aihw.gov.au/reports/chronic-musculoskeletal-conditions/rheumatoid-arthritis
Page highlights
Rheumatoid arthritis is a chronic autoimmune condition that causes inflammation, pain, swelling, stiffness and loss of function in joints, commonly in the hands.
How common is rheumatoid arthritis?
An estimated 456,000 (1.9%) people in Australia reported having rheumatoid arthritis in 2017–18.
Impact of rheumatoid arthritis
- People with rheumatoid arthritis had more than double the rates of ‘fair’ to ‘poor’ health (45%), ‘high’ to ‘very high’ psychological distress (29%) and ‘moderate’ to ‘very severe’ bodily pain (68%), compared with those without the condition.
- Rheumatoid arthritis accounted for 2.0% of total disease burden and 16% of the total burden of disease for all musculoskeletal conditions in 2023.
- In 2020–21, an estimated $966.1 million was spent on the treatment and management of rheumatoid arthritis, representing 0.6% of total health system expenditure and 6.6% of expenditure for all musculoskeletal conditions.
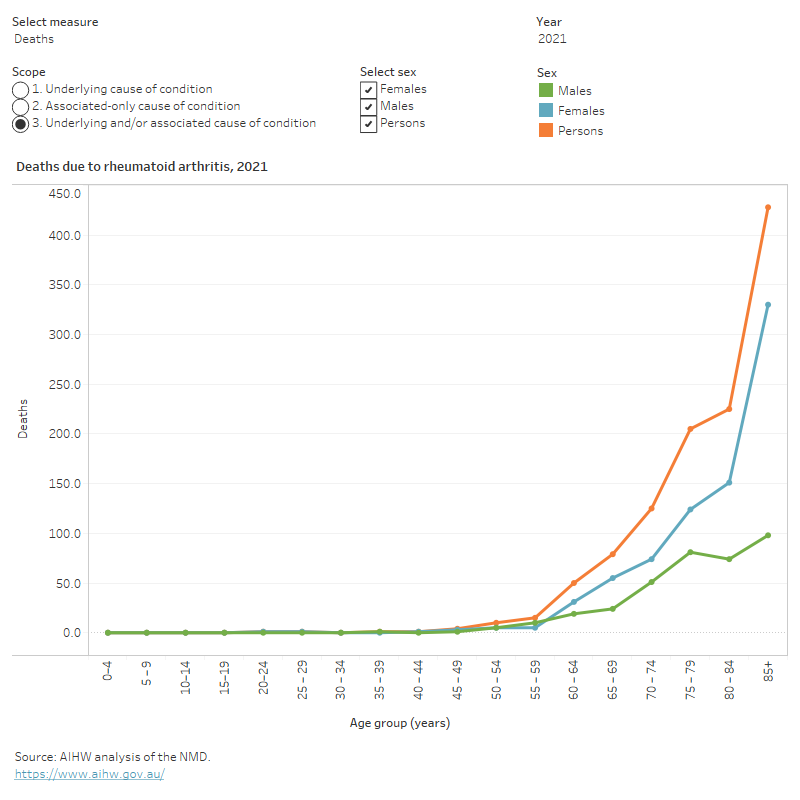
- Rheumatoid arthritis contributed to 1,145 deaths or 3.2 deaths per 100,000 population in 2021, representing 0.7% of all deaths.
Treatment and management of rheumatoid arthritis
In 2021–22, there were 10,000 hospitalisations with a principal diagnosis of rheumatoid arthritis (39 hospitalisations per 100,000 population).
Comorbidities of rheumatoid arthritis
Six of 9 comorbidities analysed were significantly more common among people with rheumatoid arthritis compared to those without – the top 3 comorbidities were back problems (36%), mental and behavioural conditions (35%), and heart, stroke and vascular disease (22%).
What is rheumatoid arthritis?
Rheumatoid arthritis is a chronic autoimmune condition characterised by inflammation of the joints, pain, swelling, stiffness and loss of function in the joints. Rheumatoid arthritis commonly affects the hand joints and both sides of the body at the same time (CDC 2019).
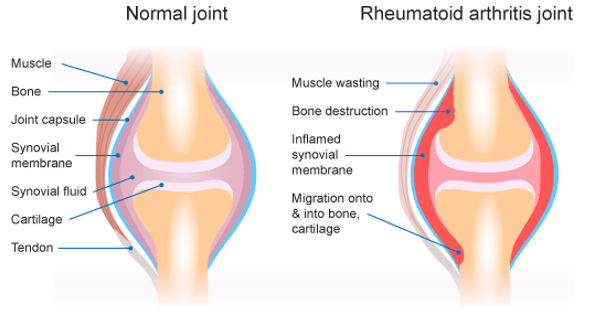
In a healthy joint, the tissue lining the joint (called the synovial membrane or joint synovium) is very thin and produces fluid that lubricates and nourishes joint tissues (RACGP 2009). In rheumatoid arthritis, the immune system attacks the synovial membrane (RACGP 2009). The synovial membrane becomes thick and inflamed, resulting in unwanted tissue growth (Figure 1). As a result, bone erosion and irreversible joint damage can occur, leading to permanent disability (RACGP 2009).
Rheumatoid arthritis is a systemic disease, affecting the whole body, including the organs. This can lead to problems with the heart, respiratory system, nerves and eyes (CDC 2019). Its cause is not well understood although there is a strong genetic component (CDC 2019). Genetic factors are estimated to contribute 50–60% of the risk of developing rheumatoid arthritis (Tobón et al. 2010).
Figure 1: Comparison of healthy joint and joint with rheumatoid arthritis
How common is rheumatoid arthritis?
An estimated 456,000 (1.9%) people in Australia reported having rheumatoid arthritis, according to the 2017–18 Australian Bureau of Statistics (ABS) National Health Survey (NHS) (ABS 2018). This represented 13% of people with any form of arthritis (excluding gout).
For more information about other forms of arthritis, see All arthritis, Osteoarthritis, Gout, and Juvenile arthritis.
Prevalence by age and sex
According to the NHS, in 2017–18, rheumatoid arthritis was:
- most common in people aged 75 years and over, although the onset of rheumatoid arthritis most frequently occurred in those aged 35–64 (AIHW 2009; Duarte-Garcia 2019)
- 1.5 times as high in females compared with males (2.3% and 1.5%, respectively) (Figure 2).
Figure 2: Prevalence of self-reported rheumatoid arthritis, by age and sex, 2017–18
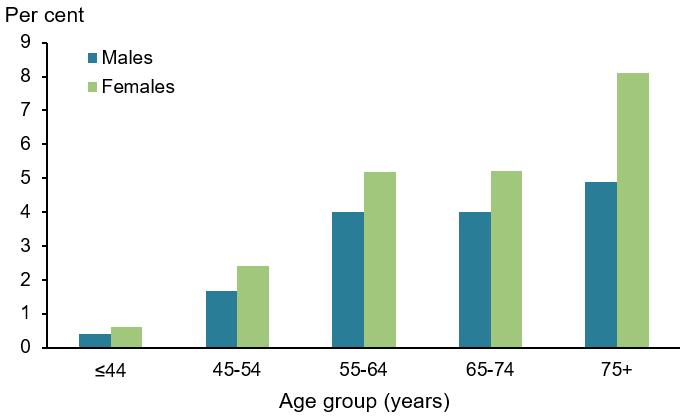
Note: Refers to people who self-reported that they were diagnosed by a doctor or nurse as having rheumatoid arthritis (current and long term) and also people who self-reported having rheumatoid arthritis.
Source: AIHW analysis of ABS 2019 (Rheumatoid arthritis 2023 Supplementary data table 1.1).
Impact of rheumatoid arthritis
Many of the symptoms of rheumatoid arthritis, such as physical limitations, pain, fatigue and mental health issues can impact a person’s ability to engage in daily activities (Radner et al. 2010).
How does rheumatoid arthritis affect quality of life?
Rheumatoid arthritis can affect a person’s ability to participate in work, hobbies and social and daily activities. Combined with the chronic pain associated with rheumatoid arthritis, this can lead to mental health issues including stress, depression and anxiety (Arthritis Australia 2017; Covic et al. 2012).
Rheumatoid arthritis is also a significant cause of physical disability. Functional limitations can become evident soon after the onset of the disease and worsen with time. Joint damage in the wrist is reported as the cause of most severe limitation even in the early stages of rheumatoid arthritis (Koevoets et al. 2013).
According to the NHS, in 2017–18, after adjusting for age, people aged 45 and over with rheumatoid arthritis were:
- less likely to describe their health as ‘excellent’ or ‘very good’, and 2.3 times as likely to report having ‘fair’ to ‘poor’ health compared with those without rheumatoid arthritis (45% and 19%, respectively) (Figure 3)
- 2.3 times as likely to experience ‘high’ to ‘very high’ levels of psychological distress compared with people without rheumatoid arthritis (29% and 13%, respectively) (Figure 4)
- 2.1 times as likely to experience ‘moderate’ to ‘very severe’ bodily pain compared with those without rheumatoid arthritis (68% and 33%, respectively) (Figure 5).
Figure 3: Self-assessed health of people aged 45 and over with and without rheumatoid arthritis, 2017–18
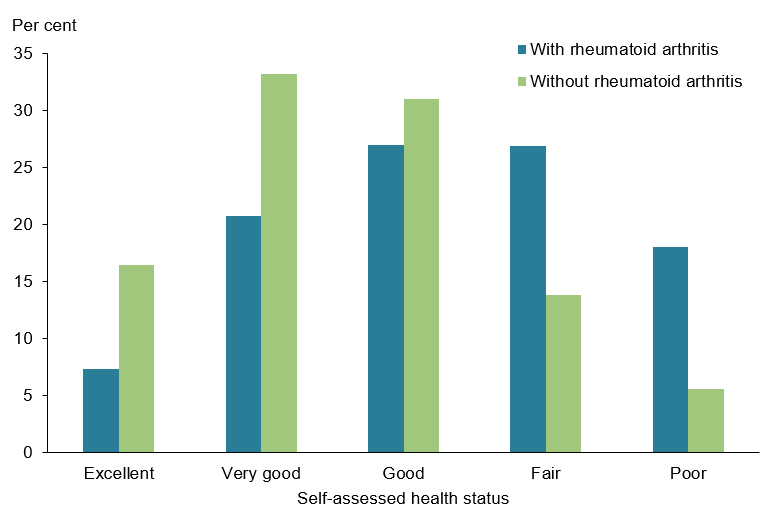
Note: Rates are age-standardised to the Australian population as at 30 June 2001.
Source: AIHW analysis of ABS 2019 (Rheumatoid arthritis 2023 Supplementary data table 2.1).
Figure 4: Psychological distress experienced by people aged 45 and over with and without rheumatoid arthritis, 2017–18
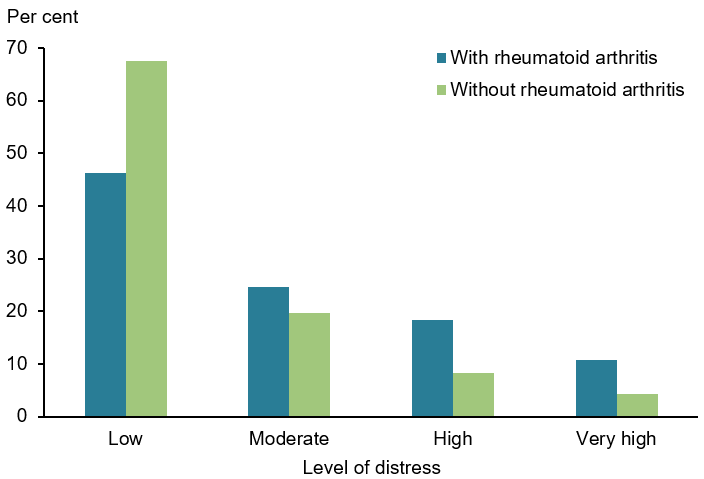
Note: Rates are age-standardised to the Australian population as at 30 June 2001.
Source: AIHW analysis of ABS 2019 (Rheumatoid arthritis 2023 Supplementary data table 2.2).
Figure 5: Pain(a) experienced by people aged 45 and over with and without rheumatoid arthritis, 2017–18
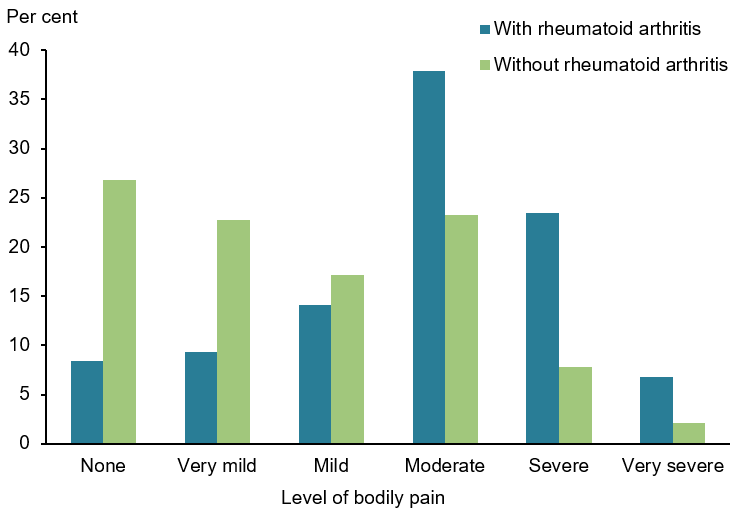
(a) Bodily pain experienced in the 4 weeks prior to interview.
Note: Rates are age-standardised to the Australian population as at 30 June 2001.
Source: AIHW analysis of ABS 2019 (Rheumatoid arthritis 2023 Supplementary data table 2.3).
Burden of disease
What is burden of disease?
Burden of disease is measured using the summary metric of disability-adjusted life years (DALY, also known as the total burden). One DALY is one year of healthy life lost to disease and injury. DALY caused by living in poor health (non-fatal burden) are the ‘years lived with disability’ (YLD). DALY caused by premature death (fatal burden) are the ‘years of life lost’ (YLL) and are measured against an ideal life expectancy. DALY allows the impact of premature deaths and living with health impacts from disease or injury to be compared and reported in a consistent manner (AIHW 2022a).
In 2023, rheumatoid arthritis accounted for 2.0% of total disease burden (DALY); 3.6% of non-fatal burden (YLD), and 0.1% of fatal burden (YLL).
Within the musculoskeletal conditions disease group, rheumatoid arthritis accounted for 15.7% of total burden (DALY); 15.7% of non-fatal burden (YLD); and 15.5% of fatal burden (YLL) (AIHW 2023a).
Variation by age and sex
In 2023, the rate of burden from rheumatoid arthritis:
- was 1.6 times as high for females compared with males (5.3 and 3.3 DALY per 1,000 population, respectively)
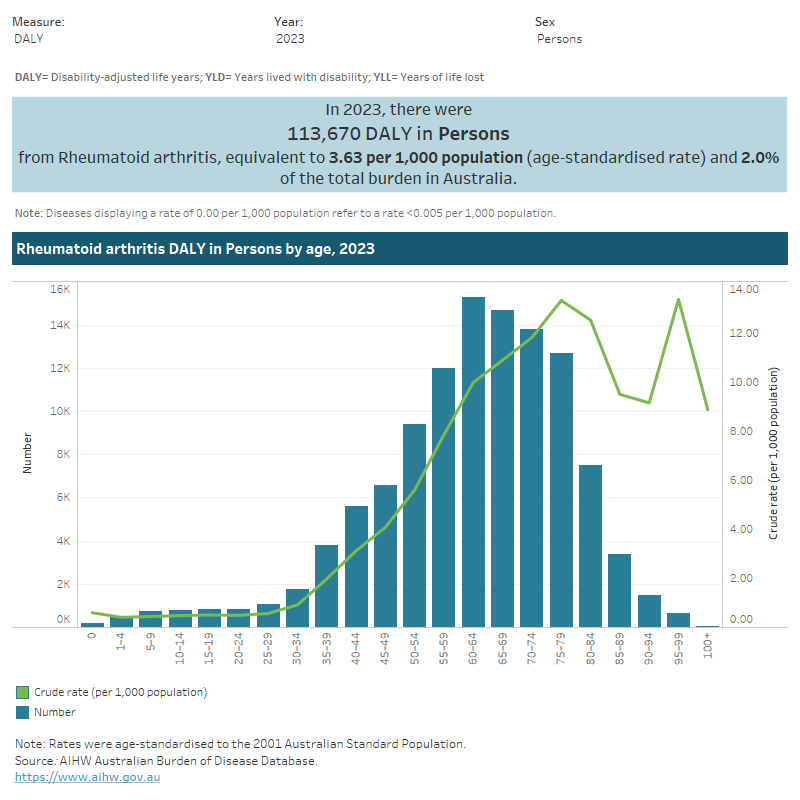
- averaged 0.6 DALY per 1,000 population for age groups below 30–34, and then rose steeply with age, reaching 13.3 DALY per 1,000 population for 75–79 years (Figure 6).
Figure 6: Burden of disease due to rheumatoid arthritis by sex, age and year
This figure shows the rate of total burden of disease for rheumatoid arthritis was highest for people aged 60–64 in 2023.
This figure shows that the rate of total burden of disease for rheumatoid arthritis was highest for females living in the lowest socioeconomic areas in 2018.

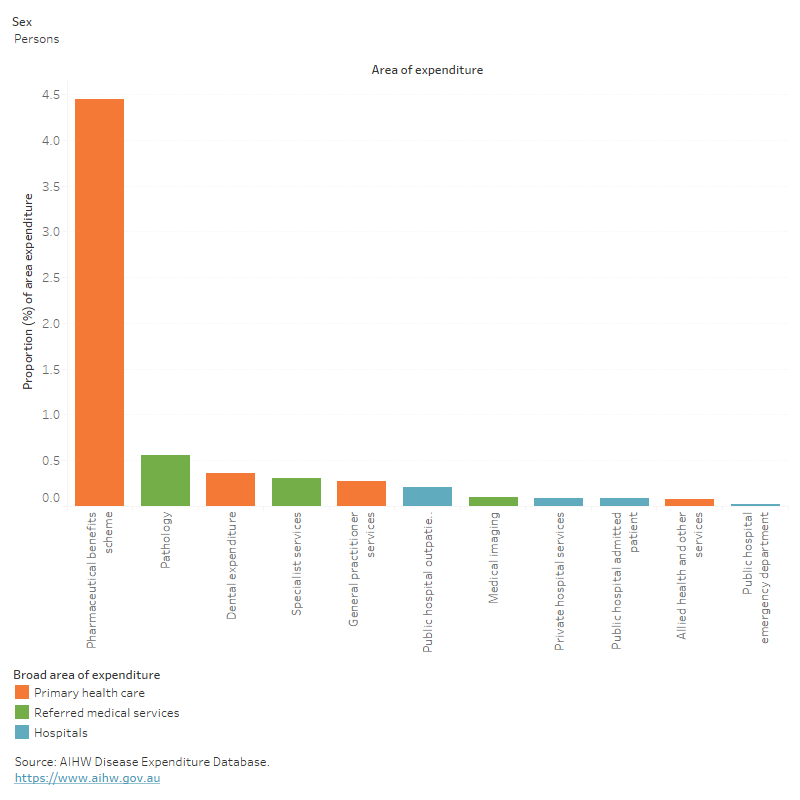
This figure shows that the primary care proportion of rheumatoid arthritis expenditure was $736 million (84%) in 2020-21.
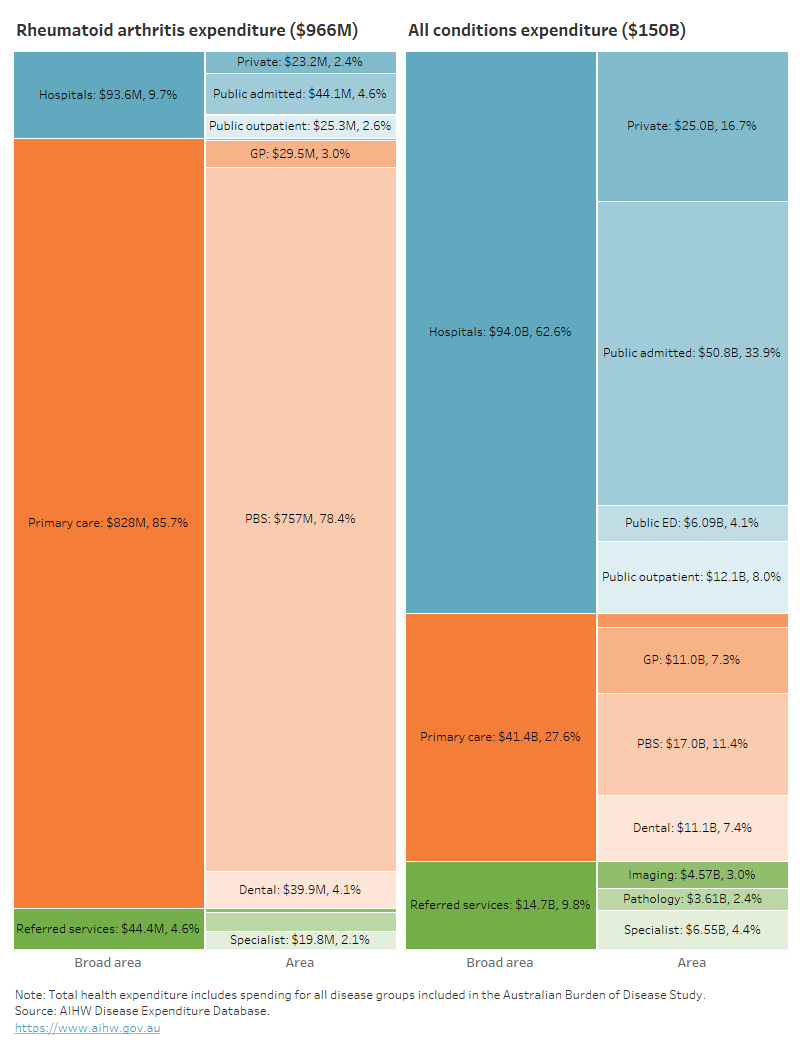
This figure shows that rheumatoid arthritis accounted for 1.0% of referred medical services expenditure in 2020–21.
This figure shows that in 2021, the rheumatoid arthritis death rate increased from 3.4 per 100,000 population in people aged 60–64 to 80 per 100,000 in those aged 85 and over.
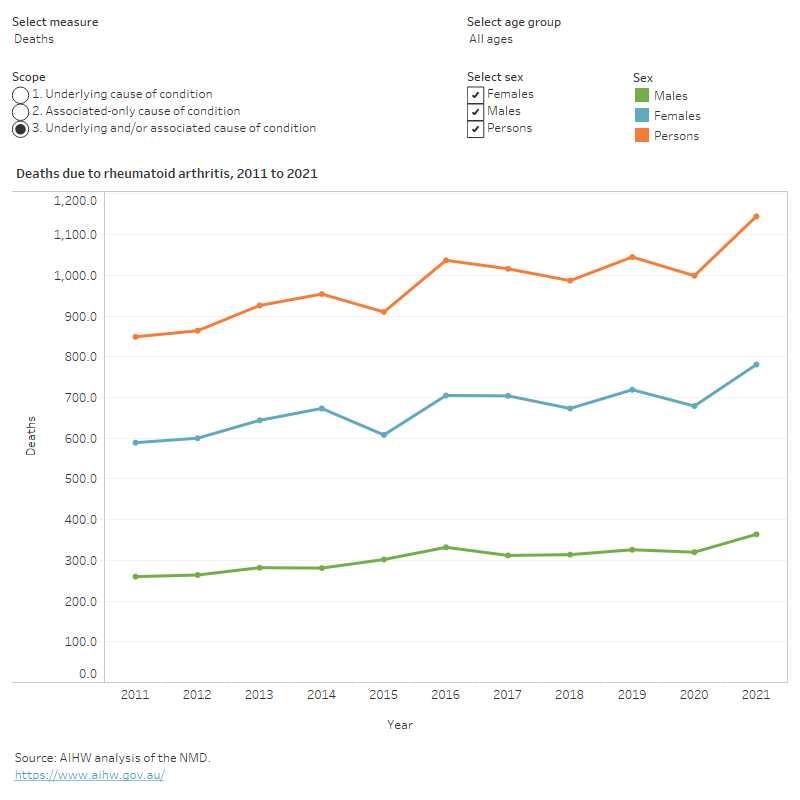
This figure shows that the female rheumatoid arthritis death rate was lowest in 2015 (5.1 per 100,000 population).
This figure shows that the hospitalisation rate for rheumatoid arthritis increased with age up to the 75–79 age group, decreasing thereafter.
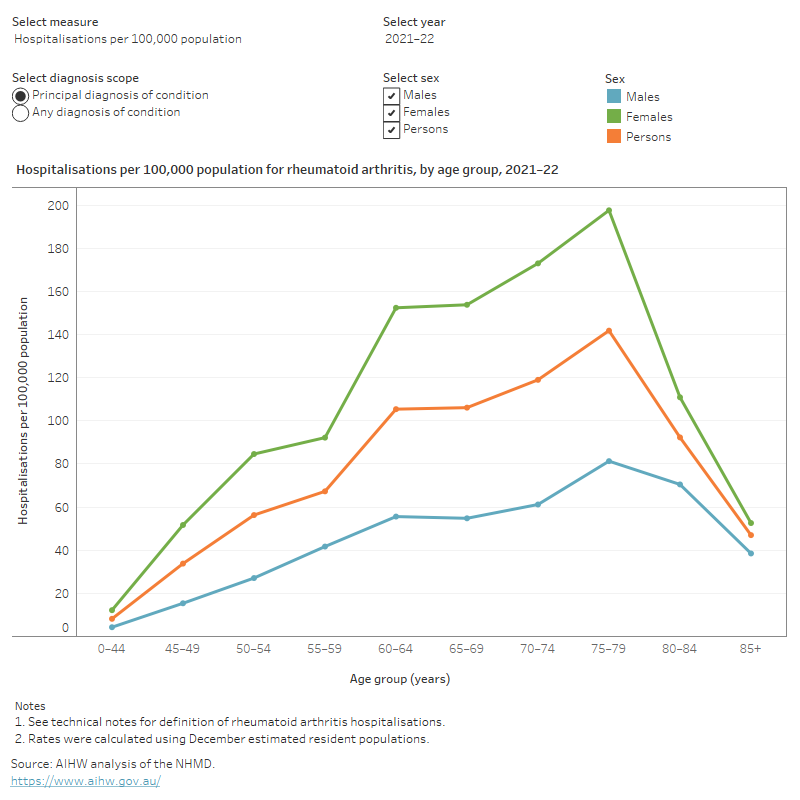
This figure shows that between 2011–12 and 2021–22, hospitalisation rates for rheumatoid arthritis were consistently higher for females compared to males.

Comorbidities of rheumatoid arthritis
People with rheumatoid arthritis often have other chronic conditions, known as a comorbidity. For this analysis, the following comorbidities were considered:
- arthritis
- asthma
- back problems
- cancer
- diabetes
- heart, stroke and vascular disease
- kidney disease
- mental and behavioural conditions
- osteoporosis or osteopenia.
According to the NHS, in 2017–18, among people aged 45 and over with rheumatoid arthritis:
- 36% also had back problems compared with 25% of people without rheumatoid arthritis
- 35% also had mental and behavioural conditions compared with 22% of people without rheumatoid arthritis
- 22% also had heart, stroke and vascular disease compared with 11% of people without rheumatoid arthritis.
Most chronic diseases are more common in older age groups. The average age of people with rheumatoid arthritis is older than the average age of the general population, therefore people with rheumatoid arthritis are more likely to have age-related comorbidities.
The rates of back problems, mental and behavioural conditions, heart, stroke, and vascular disease, asthma, osteoporosis, and COPD as comorbidities remained significantly higher for people with rheumatoid arthritis compared with those without after adjusting for age (Figure 14). There was no significant difference for diabetes, cancer or kidney disease.
It is important to note that regardless of the differences in age structures, having multiple chronic health problems is often associated with worse health outcomes (Parekh et al. 2011), in addition to a poorer quality of life (McDaid et al. 2013) and more complex clinical management and increased health costs. Rheumatoid arthritis is also associated with increased mortality due to comorbidities and related complications (Lassere et al. 2013).
Figure 14: Prevalence of other chronic conditions in people aged 45 and over, with and without rheumatoid arthritis, 2017–18
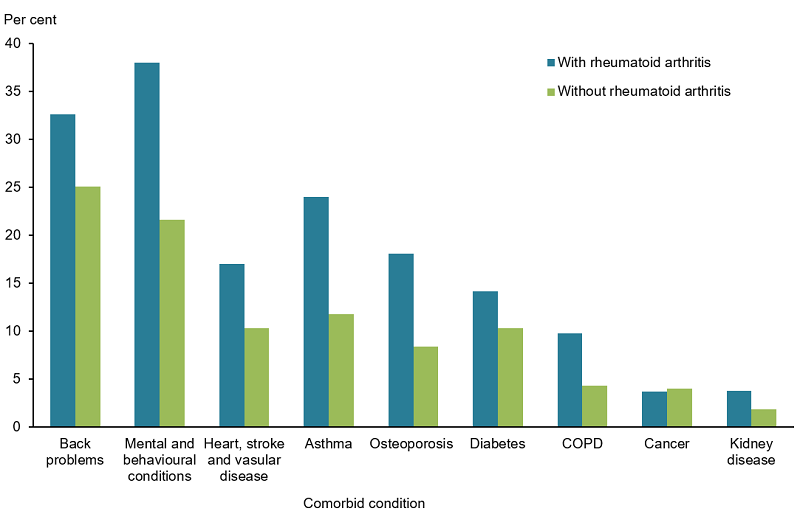
Notes:
- Rates are age-standardised to the Australian population as at 30 June 2001.
- These components do not total 100% as one person may have more than one comorbidity.
Source: AIHW analysis of ABS 2019 (Rheumatoid arthritis 2023 Supplementary data table 3.1).