Many Aboriginal and Torres Strait Islander people experience poor oral health such as multiple caries and untreated dental disease, and are less likely to have received preventive dental care (AHMAC 2017). The oral health status of Indigenous Australians, like all Australians, is influenced by many factors (see What contributes to poor oral health?) and a tendency towards unfavourable (refer to Key terms below) dental visiting patterns, broadly associated with accessibility, cost and a lack of cultural awareness by some service providers (COAG 2015; NACDH 2012).
Key terms
- Deciduous teeth: Primary or ‘baby’ teeth that erupt (that is, become visible in the mouth) during infancy. A child usually has 20 deciduous teeth.
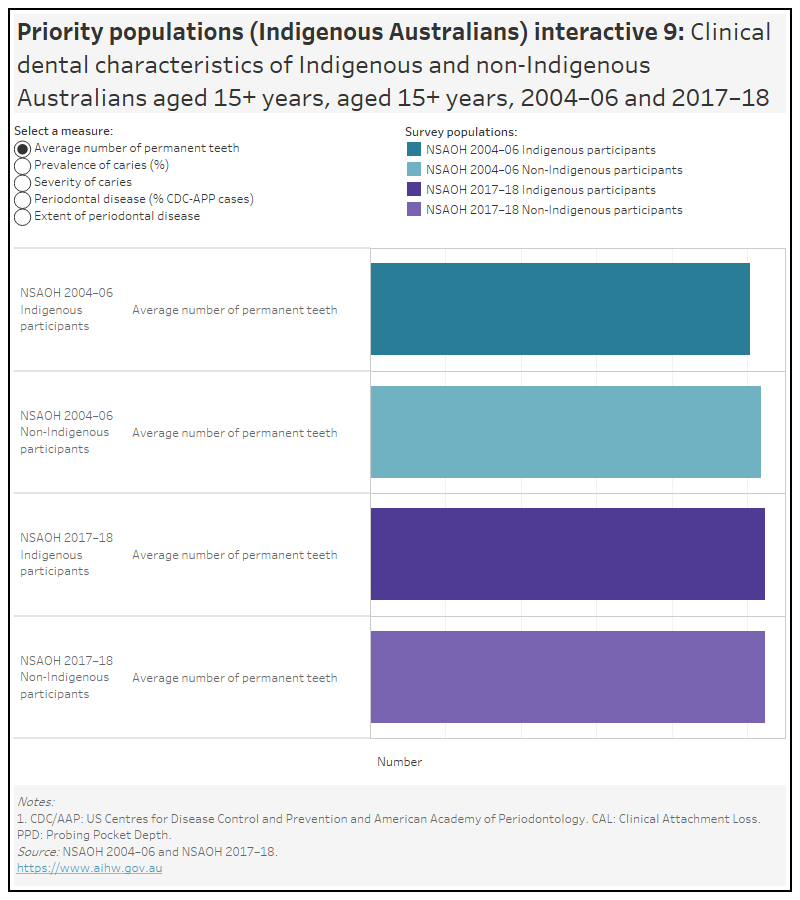
- Permanent teeth: Secondary or ‘adult’ teeth that start to erupt at around 6 years of age. A person usually has 32 permanent teeth.
- Dental caries: A disease process that can lead to cavities (small holes) in the tooth structure that compromise both the structure and the health of the tooth, commonly known as tooth decay.
- The dmfs and DMFS score: A score that counts the number of tooth surfaces that are decayed (d), missing due to caries (m) or filled because of caries (f)— ‘dmfs’ refers to deciduous teeth, ‘DMFS’ refers to permanent teeth. Each tooth was divided into five surfaces and each surface decayed or filled was counted, but each missing tooth was counted as three surfaces. Untreated decay was defined as a cavity in the surface enamel caused by the caries process, a missing surface if the tooth had been extracted because of decay and a filled surface when the filling had been placed due to decay.
- Favourable dental visiting pattern: Visiting a dentist once or more a year (usually for a check-up) and having a usual dental provider.
- Unfavourable dental visiting pattern: Visiting less than once every two years (usually for a problem), or visiting once every two years (usually for a problem) and without a regular dental provider.
- Intermediate dental visiting pattern: Visiting classified as neither favourable or unfavourable.
Aboriginal and Torres Strait Islander Health Performance Framework 2020 web report
Since 2006, Aboriginal and Torres Strait Islander Health Performance Framework (HPF) reports have provided information about Indigenous Australians’ health outcomes, key drivers of health and the performance of the health system. The HPF was designed, in consultation with Aboriginal and Torres Strait Islander stakeholder groups, to promote accountability, inform policy and research, and foster informed debate about Indigenous Australians’ health.
The Aboriginal and Torres Strait Islander Health Performance Framework 2020 web report reports on 68 measures across three domains (tiers). Measure 1.11 Oral health in Tier 1—Health status and outcomes describes the oral health of Aboriginal and Torres Strait Islander people. Data from the 2018–19 National Aboriginal and Torres Strait Islander Health Survey shows that:
- 58% of Aboriginal and Torres Strait Islander children aged 0–14 had seen a dentist in the last 12 months
- an estimated 19% of Indigenous Australians reported that they did not go to a dentist when they needed to in the previous 12 months. Reasons included: cost (42%), too busy (24%), disliking service or professional, or feeling embarrassed or afraid (22%) and waiting time too long or not available at time required (15%)
- 6% of Indigenous Australians aged 15 and over were reported to have complete tooth loss and 45% had lost at least one tooth.
Oral health outreach services for Aboriginal and Torres Strait Islander children in the Northern Territory, July 2012 to December 2022
Oral health is an important component of overall health and quality of life. Poor oral health can affect adults and children alike, causing pain, embarrassment, and even social marginalisation. For children, the effects can be long term, and carry through to adulthood.
Aboriginal and Torres Strait Islander (First Nations) children are more likely than non-Indigenous children to experience tooth decay. Several factors contribute towards the poorer oral health of First Nations children, including social disadvantage and lack of access to appropriate diet and dental services.
Since 2007, the Australian Government has helped fund oral health services for First Nations children aged under 16 in the Northern Territory. The Northern Territory Remote Aboriginal Investment Oral Health Program (NTRAI OHP) complements the Northern Territory Government Child Oral Health Program, by providing preventive (application of full-mouth fluoride varnish and fissure sealants) and clinical (tooth extractions, diagnostics, restorations and examinations) services.
The Oral health outreach services for Aboriginal and Torres Strait Islander children in the Northern Territory, July 2012 to December 2022 presents data from the NTRAI OHP (AIHW 2023).
How many First Nations children received services in the NTRAI OHP?
In 2022, full-mouth fluoride varnish services, fissure sealant applications and clinical service visits were provided to First Nations children in the Northern Territory under the NTRAI OHP. Of those children:
- 5,338 children received 6,603 full-mouth fluoride varnish services, an increase of 181 services from 2021
- 1,236 children received fissure sealant applications to 5,498 teeth during 1,346 services, an increase of 237 teeth from 2021
- 4,774 children received clinical services during 7,505 visits—such as dental assessments, fillings, extractions, or preventive services—more than twice as many visits as in 2021. This excludes 1,073 visits where only full-mouth fluoride varnish and/or fissure sealant services were provided.
Australian Indigenous children’s oral health status and use of dental care services
Data in the following sections were sourced from the National Child Oral Health Study 2012–14 (NCOHS) (Do & Spencer 2016). The NCOHS is a population-based survey which provides information on the oral health of children aged 5–14 years, who reside in all Australian states and territories. Information is collected using interviews and standardised dental examinations. A total of 26,224 children from across Australia participated in the study. The most complete information about Australians’ oral health status and their use of dental services is available via national population surveys, although these are conducted infrequently, only around once every 10 years.
Oral health status of Australian Indigenous children
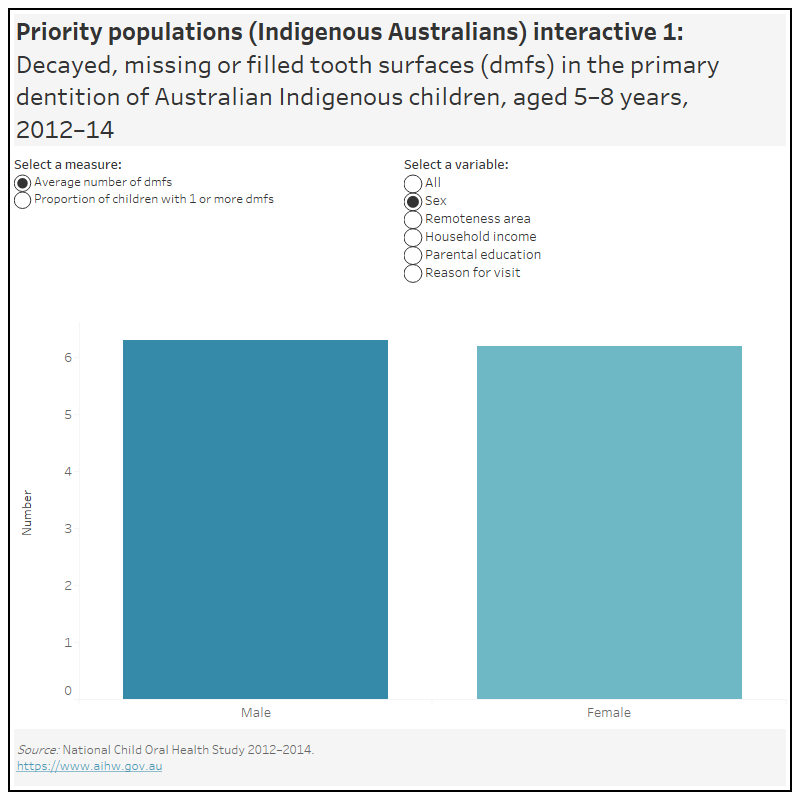
In 2012–14, Australian Indigenous children aged 5–8 years had an average number of 6.3 decayed, missing or filled tooth surfaces (dmfs) in the primary dentition
- The average number of decayed, missing or filled surfaces among Indigenous children increased as household income decreased, ranging from 0.8 dmfs in high income households, 3.1 dmfs in medium income households and 8.1 dmfs in low income households.
- Indigenous children of parents with school-level education had an average of 9.1 dmfs, whereas children of parents with vocational education had an average of 3.3 dmfs and children of parents with tertiary education had an average of 3.2 dmfs.
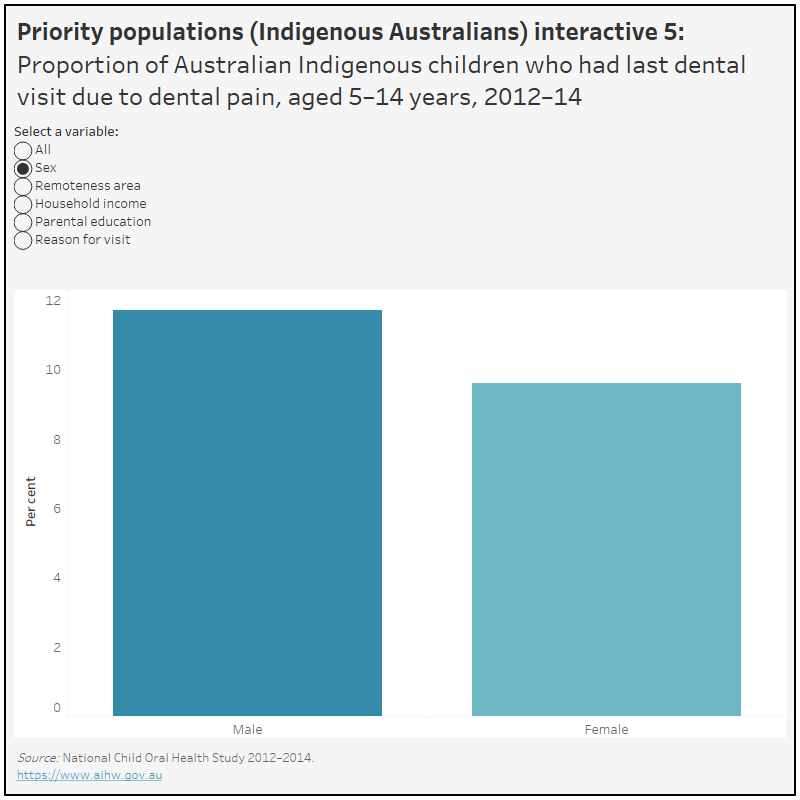
- Indigenous children who last visited the dentist for a dental problem had an average number of 13.0 dmfs, whereas those who last visited for a check-up had an average of 4.6 dmfs.
Around 6 in 10 (59%) of Australian Indigenous children aged 5–8 years had at least one tooth surface with caries experience in the primary dentition
- 57% of male and 62% of female Indigenous children had at least one tooth surface with caries experience in the primary dentition.
- The majority (80%) of Indigenous children who last visited the dentist for a dental problem had at least one tooth surface with caries experience in the primary dentition.
Explore the data using the Priority populations (Indigenous Australians) interactive 1 below.