Stroke
Page highlights:
How many Australians have had a stroke?
- In 2018, an estimated 387,000 Australians aged 15 and over (1.6% of the population) had experienced a stroke at some time in their lives.
- In 2020, there were an estimated 39,500 stroke events in Australia – more than 100 every day.
- There were around 67,900 hospitalisations where stroke was recorded as the principal diagnosis in 2021–20.
 In 2021, stroke was the underlying cause of 8,500 deaths (4.9% of all deaths and 20% of cardiovascular disease deaths).
In 2021, stroke was the underlying cause of 8,500 deaths (4.9% of all deaths and 20% of cardiovascular disease deaths).
What is stroke?
Stroke occurs when a blood vessel supplying blood to the brain either suddenly becomes blocked (ischaemic stroke) or ruptures and begins to bleed (haemorrhagic stroke).
Either may result in part of the brain dying, leading to impairment that can affect a range of activities such as speaking, thinking, movement and communication. Stroke is often fatal.
A condition related to stroke is transient ischaemic attack (TIA). TIA occurs when the blood supply to the brain is blocked temporarily. The signs are the same as for a stroke, but they disappear within a short time, and there is no evidence of damage on brain imaging. TIA is an important predictor of stroke.
Risk factors for stroke include tobacco smoking, high blood pressure, abnormal blood lipids, TIA, atrial fibrillation, diabetes and other heart disease.
Stroke is sometimes referred to as cerebrovascular disease, although cerebrovascular disease is a broader category of diseases which include stroke and other disorders of the blood vessels supplying the brain or its covering membranes. Stroke is the most common form of cerebrovascular disease.
How many Australians have had a stroke?
In 2018, an estimated 387,000 Australians aged 15 and over (1.6% of the population) had experienced a stroke at some time in their lives, based on self-reported data from the ABS Survey of Disability, Ageing and Carers (ABS 2019).
Age and sex
The prevalence of stroke was:
- higher in males (1.6%) than females (1.1%), after adjusting for differences in the age structure of the populations
- more common in older age groups – over 2 in 3 (71%) people who had a stroke were aged 65 and over. Proportions were highest for those aged 85 and over – almost 3 times as high as for those aged 65–74 (Figure 1).
Figure 1: Prevalence of self-reported stroke among persons aged 15 and over, by age and sex, 2018
The bar chart shows the prevalence of self-reported stroke by age group in 2018. Rates were highest among men and women aged 85 and over (16.0% and 12.3%).

The horizontal bar chart shows that the prevalence of self-reported stroke in 2017–18 was higher among people living in socioeconomically disadvantaged areas, but did not vary significantly by remoteness areas.

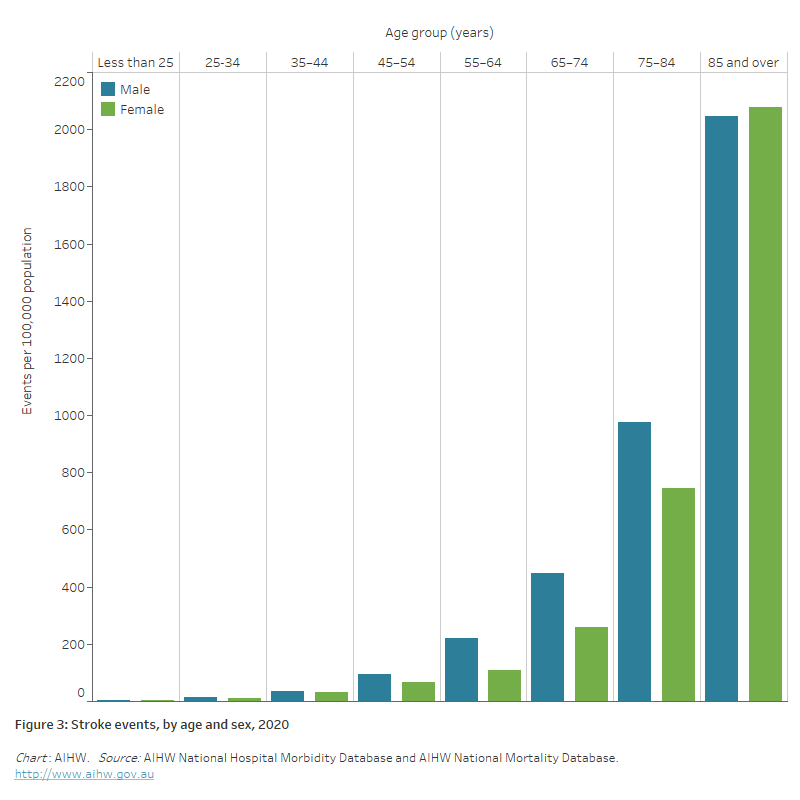
The bar chart shows the prevalence of stroke events by age group in 2020. Rates were highest among men and women aged 85 and over (2,047 and 2,077 per 100,000 population).
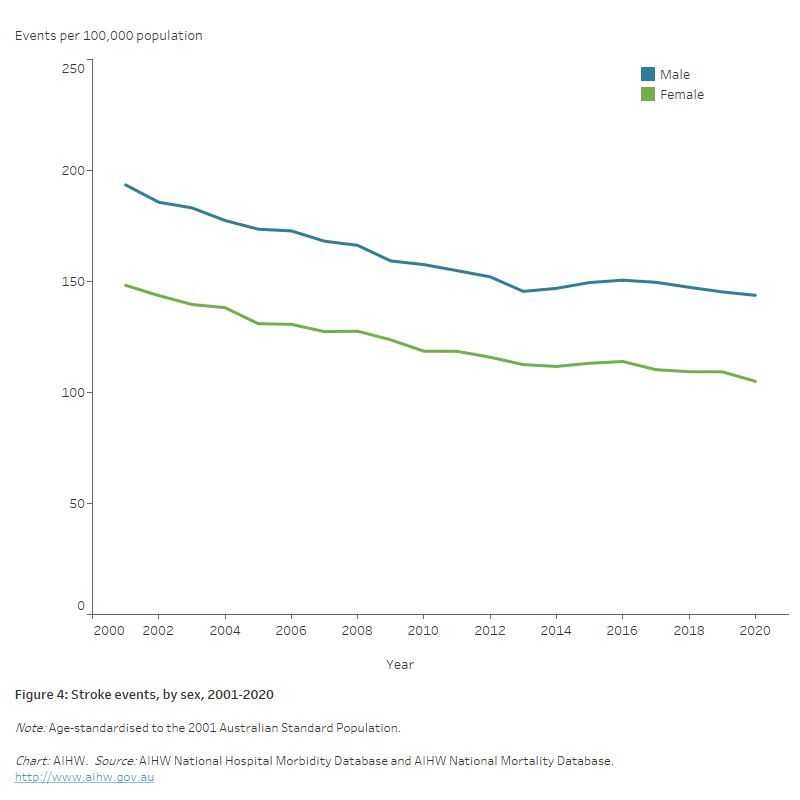
The line chart shows the decline in age-standardised rates of stroke events between 2001 and 2020, from 194 to 144 per 100,000 population for males and 148 to 105 for females.
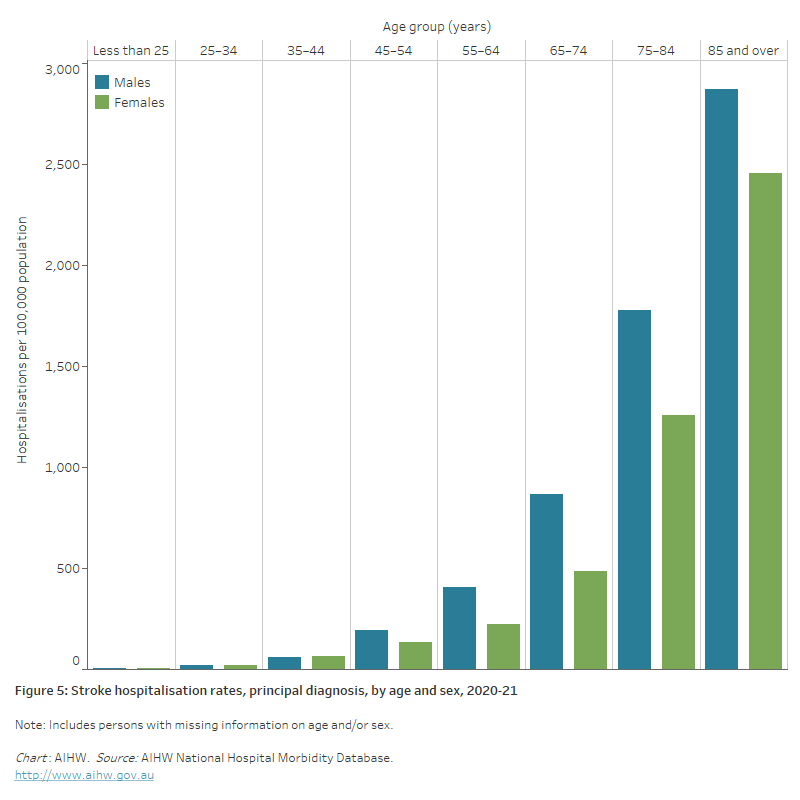
The bar chart shows stroke hospitalisation rates by age groups in 2020–21. Rates were highest among men and women aged 85 and over (2,900 and 2,500 per 100,000 population).
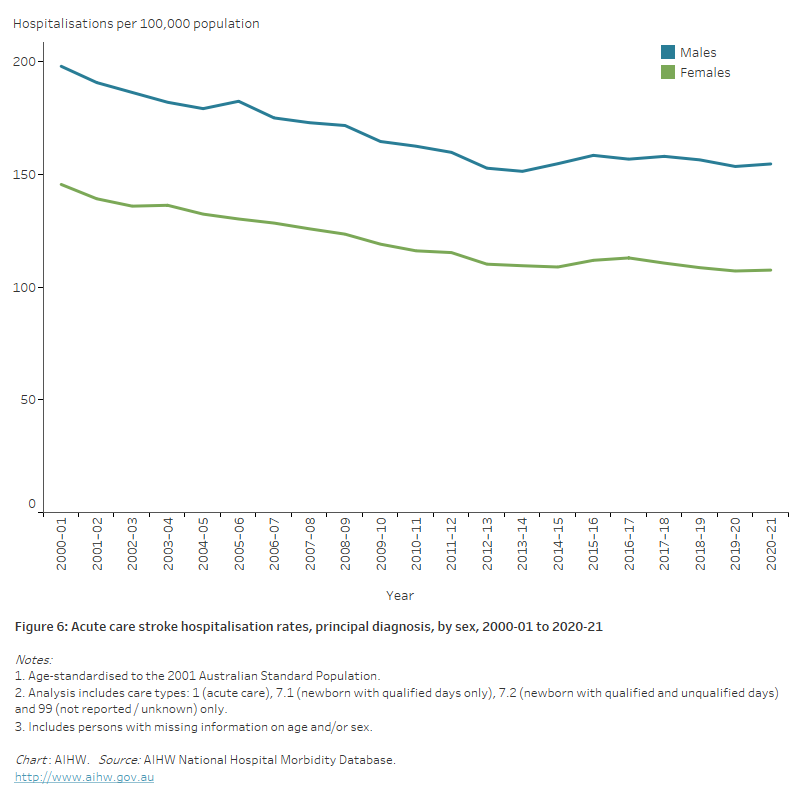
The line chart shows the decline in age-standardised rates of acute care stroke hospitalisations between 2000–01 and 2020–21, from 197 to 155 per 100,000 population for males, and from 145 to 108 for females.
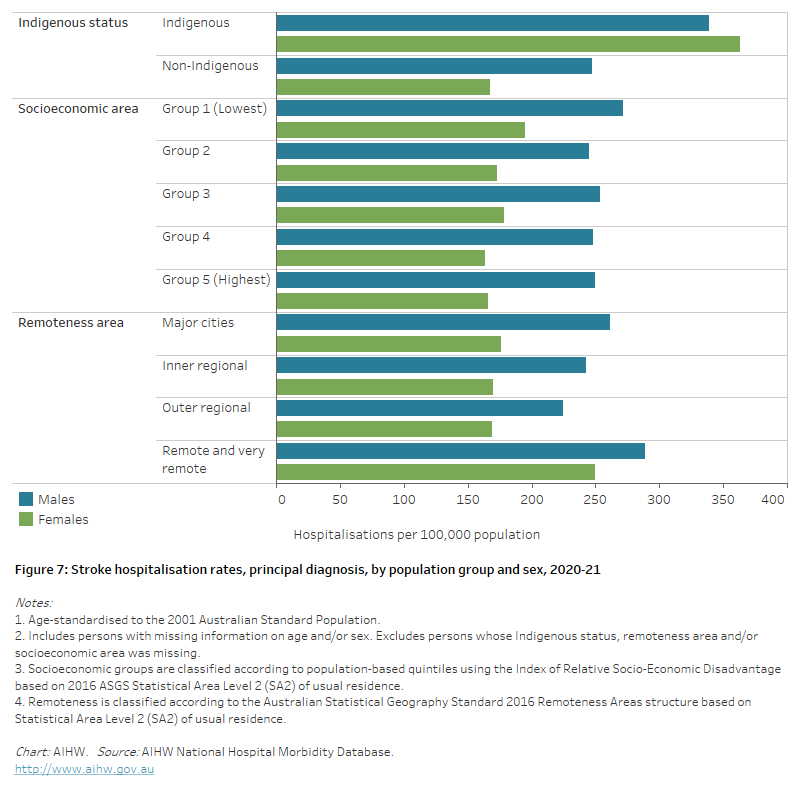
The horizontal bar chart shows that stroke hospitalisation rates in 2020–21 were higher among Indigenous Australians, people living in the lowest socioeconomic areas, and people living in remote and very remote areas.
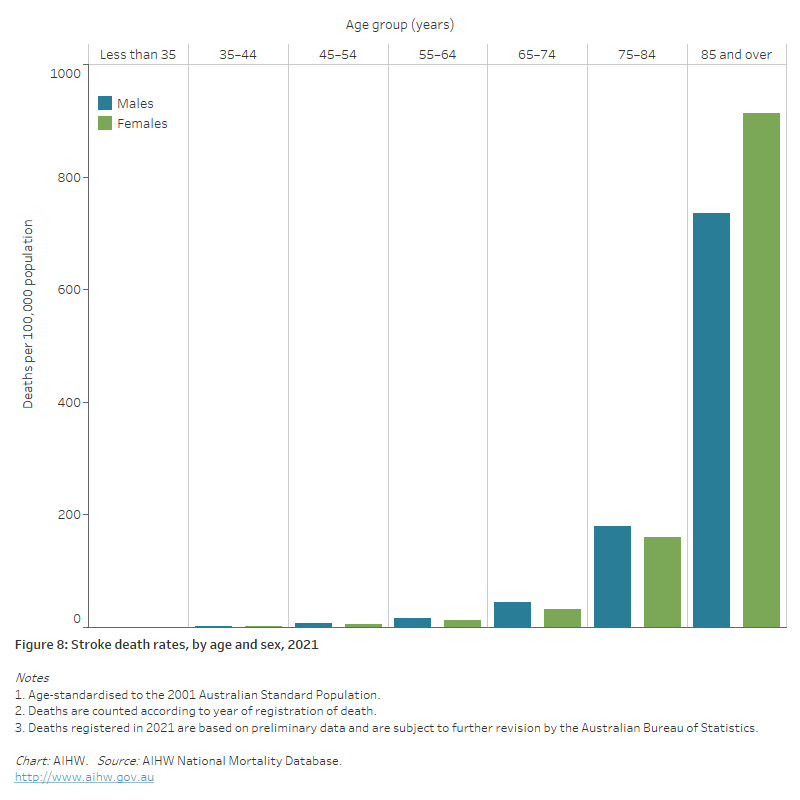
The bar chart shows stroke death rates by age groups in 2021. Rates were highest among men and women aged 85 and over (736 and 913 per 100,000 population).
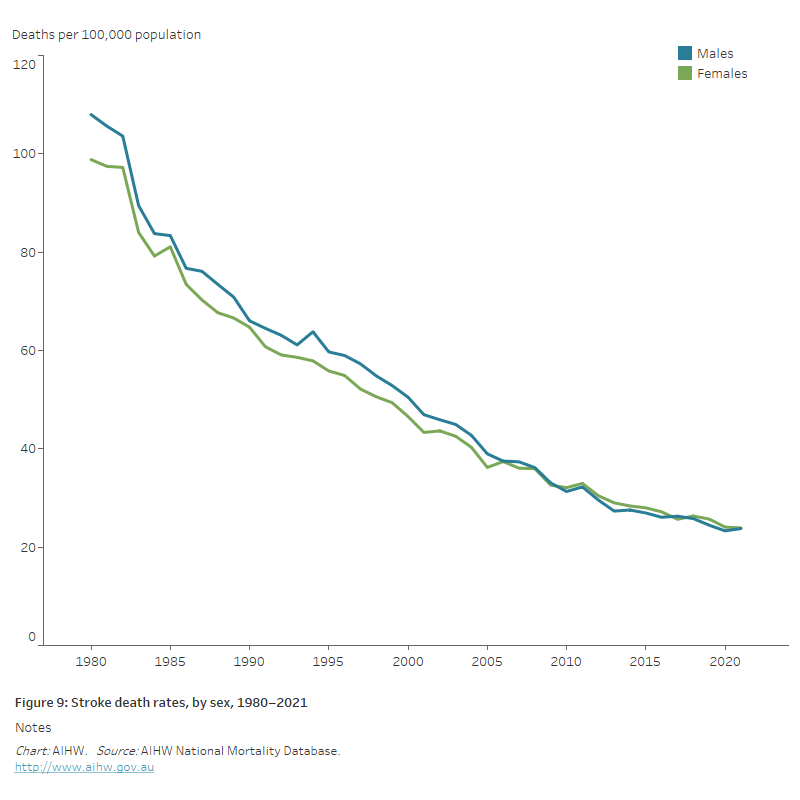
The line chart shows the decline in age-standardised coronary heart disease death rates between 1980 and 2021, from 108 to 24 per 100,000 population for males and from 99 to 24 for females.
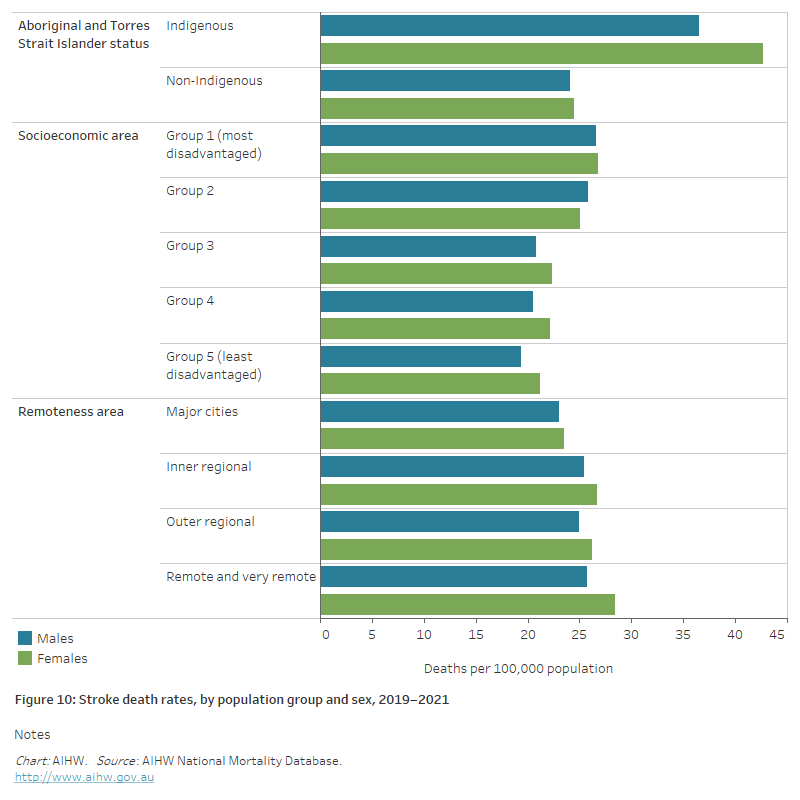
The horizontal bar chart shows that stroke death rates in 2019–2021 were higher among Indigenous Australians and people living in the lowest socioeconomic areas, but did not differ significantly by remoteness area.