Stroke
Stroke
is an Australia's health
topic
On this page:
Stroke occurs when a blood vessel supplying blood to the brain either suddenly becomes blocked (ischaemic stroke) or ruptures and begins to bleed (haemorrhagic stroke). Either may result in part of the brain dying, leading to sudden impairment that can affect a number of functions. Stroke often causes paralysis of parts of the body normally controlled by the area of the brain affected by the stroke or speech problems and other symptoms, such as difficulties with swallowing, vision and thinking.
Stroke can be prevented because many of its risk factors are modifiable. These include:
- biomedical risk factors such as high blood pressure and high blood cholesterol
- physical activity
- diet
- overweight and obesity
- smoking.
Stroke contributes to premature death, disability, and preventable hospitalisations. As a result of the substantial impact of stroke on the Australian population, a National Strategic Action Plan for Heart Disease and Stroke has been developed. The action plan aims to reflect priorities and identify implementable actions to reduce the impact of stroke in the community.
How common is stroke?
In 2018, an estimated 387,000 people aged 15 years and over – 214,000 males and 173,000 females – had had a stroke at some time in their lives, based on self-reported data from the Australian Bureau of Statistics (ABS) 2018 Survey of Disability, Ageing and Carers (ABS 2019). The estimated prevalence of stroke was similar in 2003 (1.7%) and 2018 (1.3%) (ABS 2019; AIHW 2013).
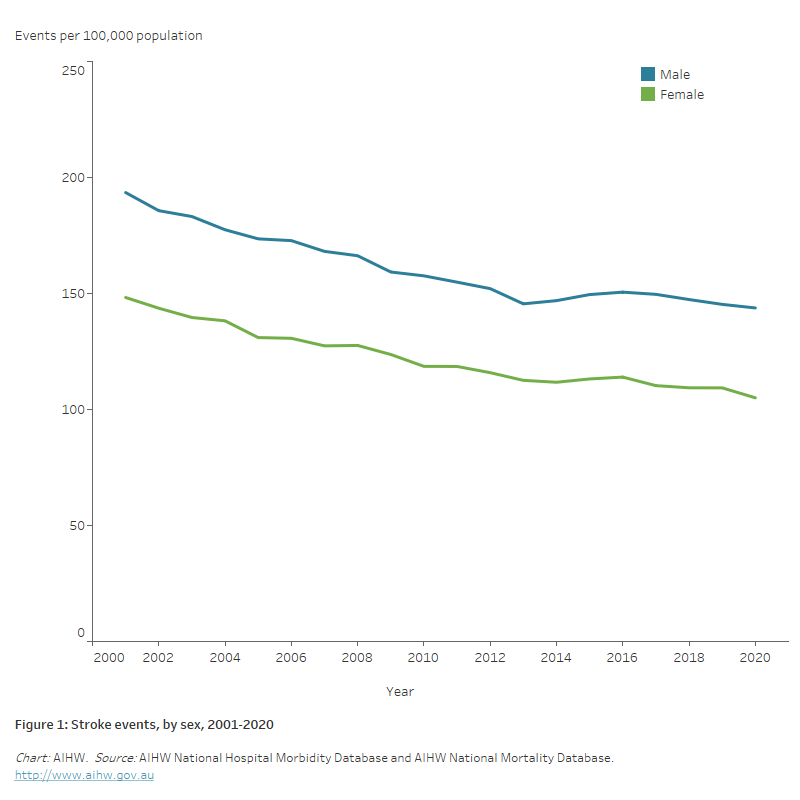
In 2020, there were around 39,500 stroke events (21,000 among males and 18,500 among females) – more than 100 every day. The stroke event rate fell by one quarter (27%) between 2001 and 2020, from an age-standardised rate of 169 to 124 per 100,000 population (Figure 1).
Figure 1: Stroke events, by sex, 2001–2020
The chart provides the number and rate of stroke events between 2001 and 2020. The age-standardised rate of stroke events decreased by 26% for males (from 194 to 144 per 100,000 population), and by 29% for women (from 148 to 105 per 100,000 population).
Impact
Deaths
In 2021, stroke was recorded as the underlying cause of 8,500 deaths, accounting for 4.9% of all deaths in Australia.
Stroke was one of the 5 leading causes of death in Australia – on average, 23 Australians died of stroke each day in 2021.
Rates of death increase with age – in 2021, rates among males and females aged 85 and over (736 and 913 per 100,000 population) were 4 and 6 times as high as rates among males and females aged 75–84 years (179 and 161 per 100,000 population).
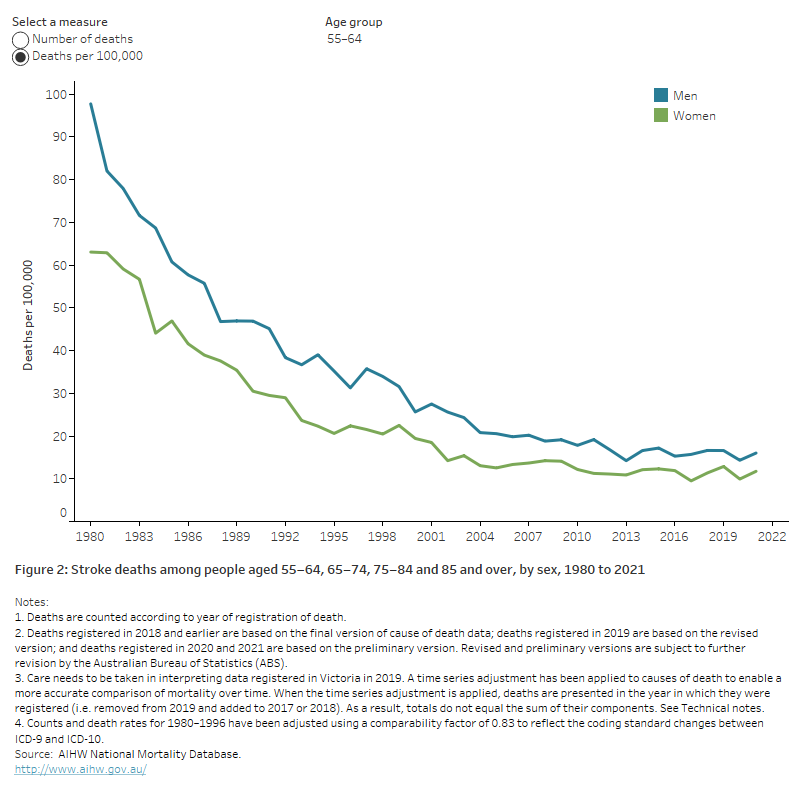
Between 1980 and 2021, death rates for stroke have fallen by three-quarters – from 108 to 24 per 100,000 population for males, and from 99 to 24 per 100,000 population for females. The rate of decline has remained steady in people aged 75 and over but has slowed among younger age groups (Figure 2).
Falling stroke death rates have been driven by a number of factors, including improvements in some risk factors such as lower rates of tobacco smoking, an increased use of blood pressure–lowering drugs, treatment to prevent blood clots, access to stroke units in hospitals and other advances in medical care (AIHW 2013).
See ‘Chapter 4 Changing patterns of mortality in Australia since 1900’ in Australia’s health 2022: data insights.
Figure 2: Stroke deaths among people aged 55-64, 65-74, 75-84 and 85 and over, by sex, 1980 to 2021
The chart shows the number and rate of deaths from stroke for males and females aged 55-64, 65-74, 75-84 and 85 and over, from 1980 to 2021. Stroke death rates fell substantially in each age group – for example, from 938 to 179 deaths per 100,000 population for men aged 75–84, and from 871 to 161 for women aged 75–84.
Burden of disease
Burden of disease refers to the quantified impact of living with and dying prematurely from a disease or injury and is measured using disability-adjusted life years (DALY). One DALY is equivalent to one year of healthy life lost.
In 2023, stroke accounted for 2.2% of the total burden of disease in Australia and was the 12th leading specific cause of disease burden (AIHW 2023a).
Stroke ranks high in disease burden among older people – for age 85 and over, it accounted for 5.1% of the burden in males and 5.8% of the burden in females.
The total burden of disease due to stroke decreased by 53% between 2003 and 2023 after adjusting for age, from 7.4 to 3.5 DALY per 1,000 population. This included a 56% decline in the fatal burden and a 23% decline in the non-fatal burden.
See Burden of disease.
Expenditure
In 2020–21, the estimated health system expenditure on stroke was more than $983.8 million. The greatest cost was for public hospital admitted patient services ($633.6 million) followed by private hospital services ($115.7 million) (AIHW 2023b).
See Health expenditure.
Treatment and management
Emergency departments
There were 41,100 presentations to Australian public hospital Emergency Departments with a principal diagnosis of stroke in 2020–21. Of these, 34,000 (83%) were admitted to the hospital to which they presented, 4,400 (11%) were referred to another hospital for admission, and 2,200 (5%) departed without being admitted or referred (AIHW 2022c).
Hospitalisations
In 2020–21, there were 41,300 acute care hospitalisations with a principal diagnosis of stroke, at a rate of 161 per 100,000 population (AIHW 2022b). Acute care hospitalisation rates were higher among males than females (1.4 times as high), and most hospitalisations (73%) were for people aged 65 and over.
Between 2000–01 and 2020–21, the age-standardised rate of hospitalisation for acute care stroke fell by 23%, from 170 to 130 per 100,000 population.
See Hospitals.
Rehabilitation
Stroke rehabilitation helps stroke survivors to relearn and maintain their skills and functioning. It also seeks to protect them from developing new medical problems.
- In 2019–20, stroke patients in hospital rehabilitation care had an average length of stay of 14 days.
- Of a group of 2,800 stroke survivors assessed before hospital discharge in 2019, 64% were referred for further rehabilitation in the community (Stroke Foundation 2020).
Variation between population groups
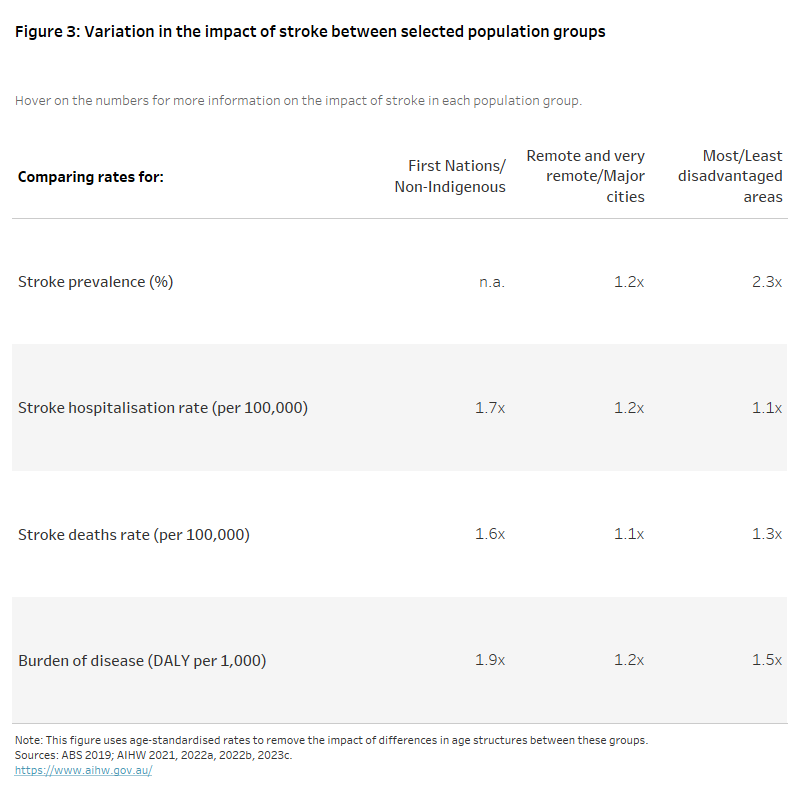
The impact of stroke varies between population groups, with age-standardised rates higher among First Nations people than among non-Indigenous Australians for both hospitalisation (1.7 times as high) and death (1.8 times as high) (Figure 3).
Age-standardised death rates and burden of disease were both 1.2 times as high in Remote and very remote areas as in Major cities. The rate of death for stroke was 1.3 times as high in the lowest socioeconomic areas as in the highest.
The figure shows the age-standardised rate ratio of stroke prevalence (2018), hospitalisation (2020–21), death (2021) and burden of disease (2018) among selected population groups.
Rates were higher among First Nations people than among non-Indigenous Australians for both hospitalisation (1.7 times as high) and death (1.6 times as high). Death rates and burden of disease were both 1.2 times as high in Remote and very remote areas as in Major cities. The rate of death for stroke was 1.3 times as high in the lowest socioeconomic areas as in the highest.
COVID-19 and stroke
People who have had a stroke are at a higher risk of severe symptoms and complications from COVID-19. People with COVID-19 are also at greater risk of stroke (Nannoni et al. 2021).
The first wave of the pandemic negatively impacted access to specialised stroke units in hospitals, with fewer resources available for treatment, leading to concerns about reduced quality of care for stroke patients (Cadilhac et al. 2022).
Australian Bureau of Statistics (ABS) provisional mortality statistics indicate that there were 9,100 doctor-certified deaths due to cerebrovascular diseases (including stroke) during 2020, rising to 9,300 in 2021 and 9,300 in 2022 (ABS 2023).
The increase in cerebrovascular disease deaths reverses a historical decline, with the number of deaths in 2022 being 2.2% higher than in 2020.
Where do I go for more information?
For more information on stroke, see: Stroke.
ABS (Australian Bureau of Statistics) (2019) Survey of Disability, Ageing and Carers, 2018, ABS, Australian Government, accessed 1 February 2022.
ABS (2023) Provisional mortality statistics ABS, Australian Government, accessed 31 March 2023.
AIHW (Australian Institute of Health and Welfare) (2013) Stroke and its management in Australia: an update, AIHW, Australian Government, accessed 1 February 2022.
AIHW (2021) Australian Burden of Disease Study 2018: Interactive data on disease burden, AIHW, Australian Government, accessed 16 March 2023.
AIHW (2022a) Australian Burden of Disease Study: impact and causes of illness and death in Aboriginal and Torres Strait Islander people 2018, AIHW, Australian Government, accessed 11 March 2022.
AIHW (2022b) National Hospital Morbidity Database, Findings based on unit record analysis, AIHW, Australian Government, accessed 1 September 2022.
AIHW (2022c) National Non-admitted Patient Emergency Department Care Database, Findings based on unit record analysis, AIHW, Australian Government, accessed 1 September 2022.
AIHW (2023a) Australian Burden of Disease Study 2023, AIHW, Australian Government, accessed 14 December 2023.
AIHW (2023b) Health system spending on disease and injury in Australia 2020-21, AIHW, Australian Government, accessed 29 November 2023.
AIHW (2023c) National Mortality Database, Findings based on unit record analysis, AIHW, Australian Government, accessed 23 March 2023.
Cadilhac DA, Kim J, Cloud G, Anderson CS, Tod EK, Breen SJ, Faux S, Kleinigh T, Castley H, Lindley RJ, Middleton S, Yan B, Hill K, Jones B, Shah D, Jaques K, Clissold B, Campbell B and Lannin NA on behalf of the AuSCR COVID-19 Reporting Consortium Group (2022) ‘Effect of the Coronavirus Disease 2019 pandemic on the quality of stroke care in stroke units and alternative wards: a national comparative analysis’, Journal of Stroke, 24:79–87, doi:10.5853/jos.2021.02530.
Nannoni S, de Groot R, Bell S and Markus HS (2021) ‘Stroke in COVID-19: a systematic review and meta-analysis’, International Journal of Stroke, 16:137–149, doi:10.1177/1747493020972922.
Stroke Foundation (2020) National Stroke Audit—rehabilitation services report 2020, Stroke Foundation, Melbourne, accessed 1 February 2022.