Congenital heart disease
Page highlights:
How many Australians have congenital heart disease?
- In Australia, an estimated 65,000 children and adults live with congenital heart disease.
- In 2020–21, there were around 5,900 hospitalisations in Australia where congenital heart disease was the principal diagnosis.
 In 2021, congenital heart disease caused 79 deaths in infants aged under 1 year, equivalent to 7.8% of all infant deaths.
In 2021, congenital heart disease caused 79 deaths in infants aged under 1 year, equivalent to 7.8% of all infant deaths.
What is congenital heart disease?
Congenital heart disease is a general term for any defect of the heart, heart valves or central blood vessels that is present at birth.
It can take many forms, such as holes between the pumping chambers of the heart, valves that do not open or close properly and narrowing of major blood vessels such as the aorta and pulmonary artery. Congenital heart disease can range from simple to complex, and more than 1 anomaly can occur in the same heart.
Diagnosis usually occurs within the first month of life. Common symptoms include bluish lips, fingers and toes, breathlessness or trouble breathing, low birth weight, difficulty feeding and gaining weight, and chest pain.
Most congenital heart disease is multifactorial and arises through combinations of genetic and environmental factors. Some of the known risk factors include a family history of congenital heart disease, maternal illnesses such as rubella (German measles), misuse of alcohol, illicit drugs and medications, and maternal health factors such as preeclampsia and poorly controlled diabetes.
The National Strategic Action Plan for Childhood Heart Disease aims to reduce the impact of congenital heart disease and other childhood heart diseases in Australia. It outlines priority areas and actions to help people with Childhood Heart Disease live longer, healthier and more productive lives.
How many Australians have congenital heart disease?
National rates of congenital heart disease are not routinely reported. Globally, an estimated 9.4 in every 1,000 live births were affected by congenital heart disease during the period 2010–2017 (Liu et al. 2019).
- In Australia, an estimated 65,000 children and adults live with congenital heart disease (Department of Health 2019).
- A number of Australian jurisdictions publish their incidence of congenital heart disease, noting that data collection methods vary (AIHW 2019, 2022). Ventricular septal defect was the most commonly reported congenital heart disease, followed by atrial septal defect and patent ductus arteriosus.
Main types of congenital heart disease
Ventricular septal defect – a hole in the muscle wall between the right and left ventricles.
Atrial septal defect – a hole in the muscle wall between the right and left atria.
Patent ductus arteriosus – where the ductus arteriosus, the connection between the aorta and pulmonary artery, fails to close after birth.
Tetralogy of Fallot – a condition that consists of 4 heart anomalies: ventricular septal defect, a narrowing of the outflow tract into the pulmonary artery, an enlarged aorta and thickening of the muscle wall of the right ventricle.
Transposition of great vessels – a condition that is usually characterised by the aorta arising from the right ventricle and the pulmonary artery from the left ventricle.
Coarctation of the aorta – narrowing of the aorta.
Aortic stenosis – obstruction of the aorta. This can be due to a narrowing of the aorta or a problem with the aortic valve.
Hypoplastic left heart syndrome – where the left ventricle is small and functionally inadequate.
Pulmonary atresia – a condition in which there is no pulmonary valve and no blood flow to the pulmonary artery.
Hospitalisations
In 2020–21, there were around 5,900 hospitalisations in Australia where congenital heart disease was the principal diagnosis – a rate of 23 hospitalisations per 100,000 population.
Age and sex
In 2020–21, where congenital heart disease was recorded as the principal diagnosis, hospitalisation rates:
- were similar for males and females after adjusting for differences in the age structure of the populations
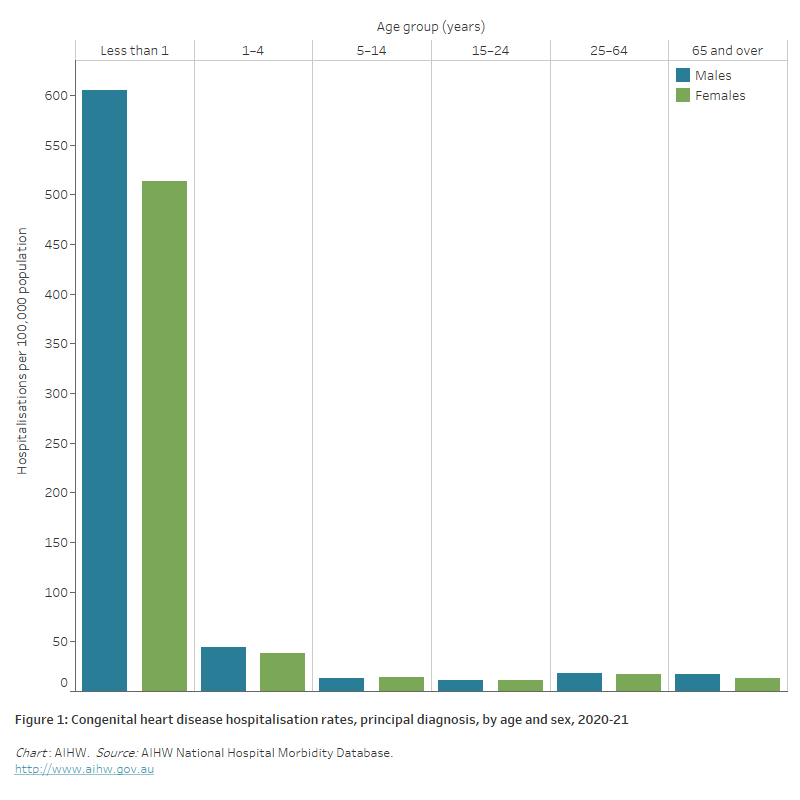
- were highest for infant boys and girls (605 and 513 per 100,000 population), followed by boys and girls aged 1–4 (45 and 39 per 100,000 population)
Unlike many other cardiovascular conditions, the number and rate of hospitalisation for congenital heart disease declines with age (Figure 1).
Figure 1: Congenital heart disease hospitalisation rates, principal diagnosis, by age and sex, 2020–21
The bar chart shows in 2020–21 congenital heart disease hospitalisation rates were highest among boys and girls aged less than 1, at 605 and 513 per 100,000 population, respectively.
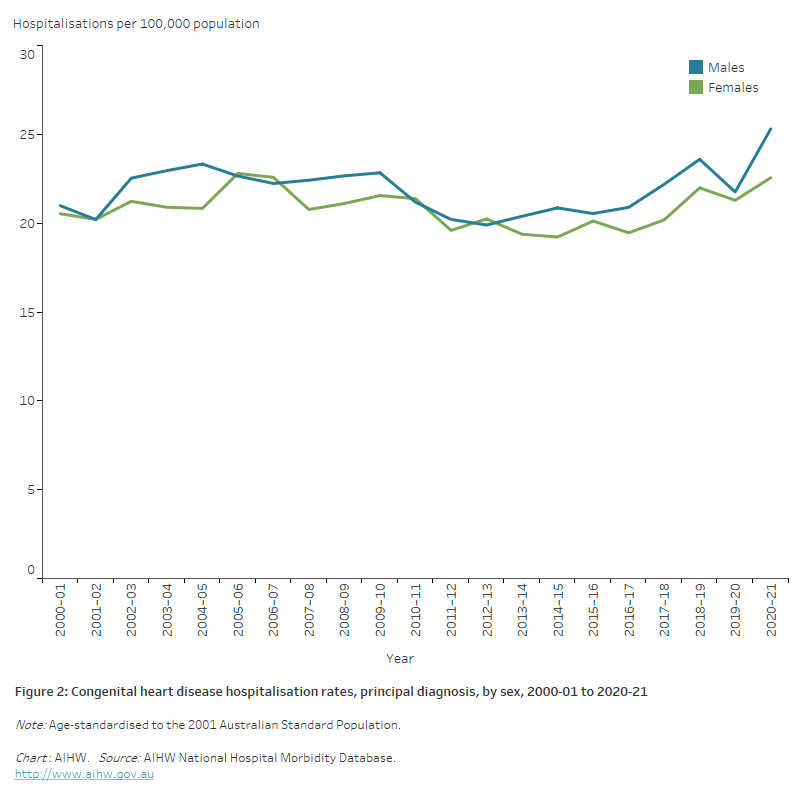
The line chart shows age-standardised congenital heart disease hospitalisation rates remained relatively stable between 2000–01 and 2020–21 with males recording 20–25 and females recording 19–23 hospitalisations per 100,000 population across the period.
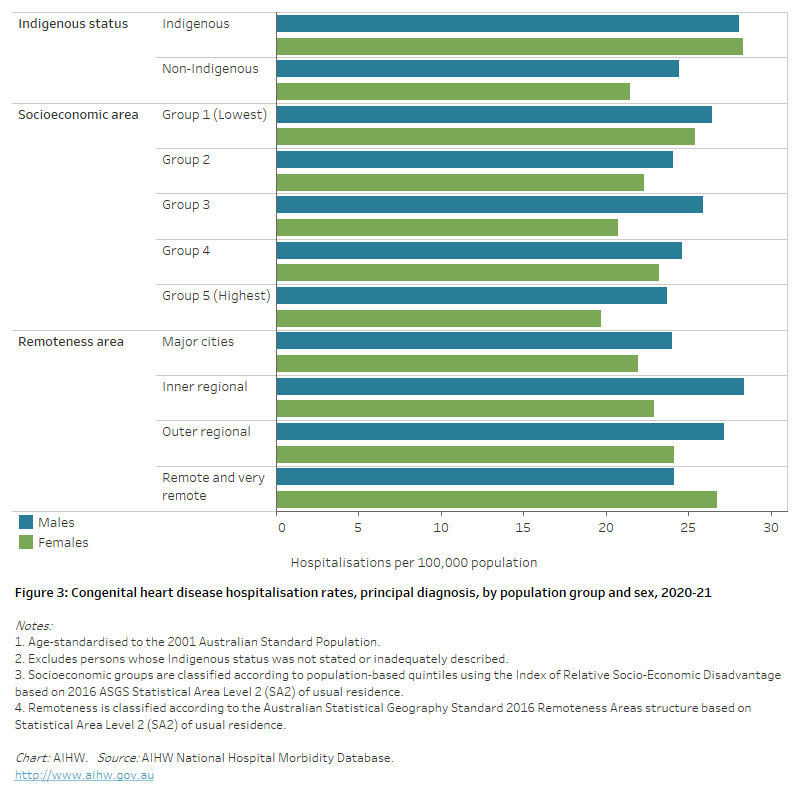
The horizontal bar chart shows that variation in age-standardised congenital heart disease hospitalisation rates among population groups was largely driven by higher rates among females. Rates were higher among Indigenous females than non-Indigenous females and females living in the lowest socioeconomic areas and Remote and very remote areas.
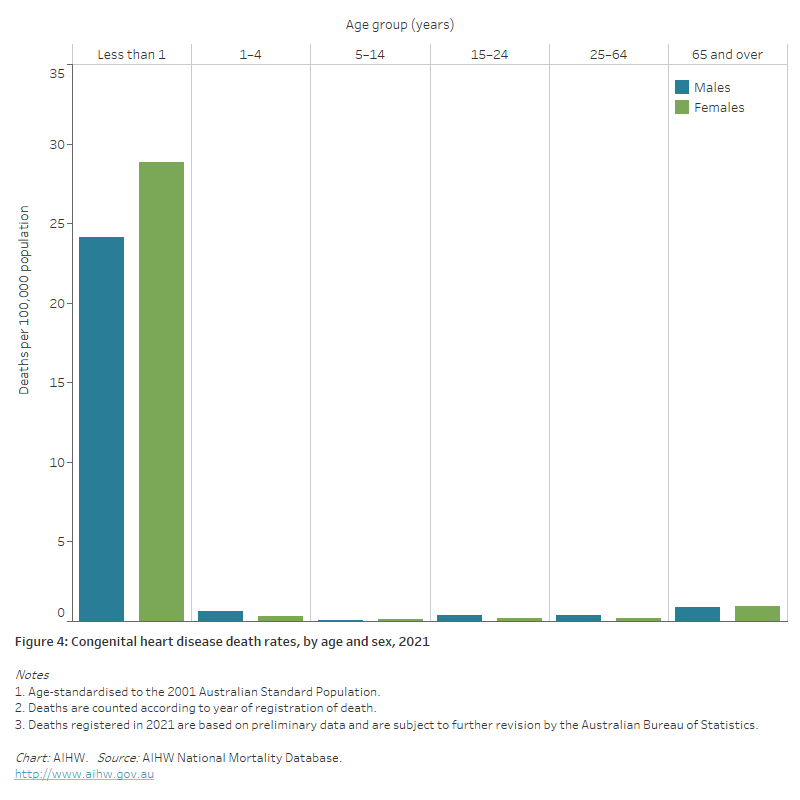
The bar chart shows in 2021 congenital heart disease death rates were highest among boys and girls aged less than 1, at 24 and 29 deaths per 100,000 population, respectively.
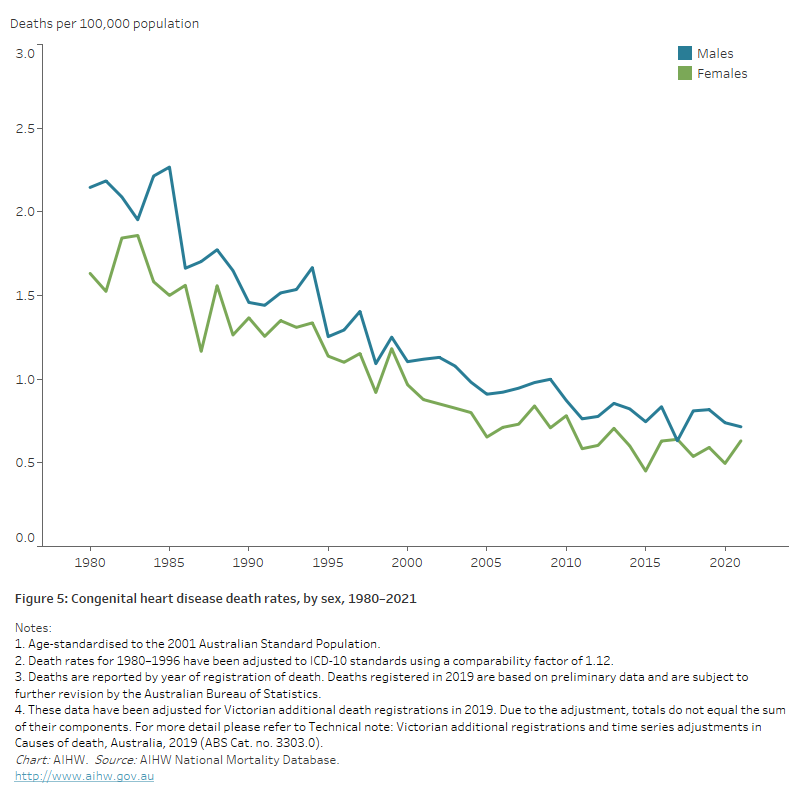
The line chart shows age-standardised congenital heart disease death rates declined between 1980 and 2021, from 2.1 to 0.7 and 1.6 to 0.6 per 100,000 population for males and females, respectively.
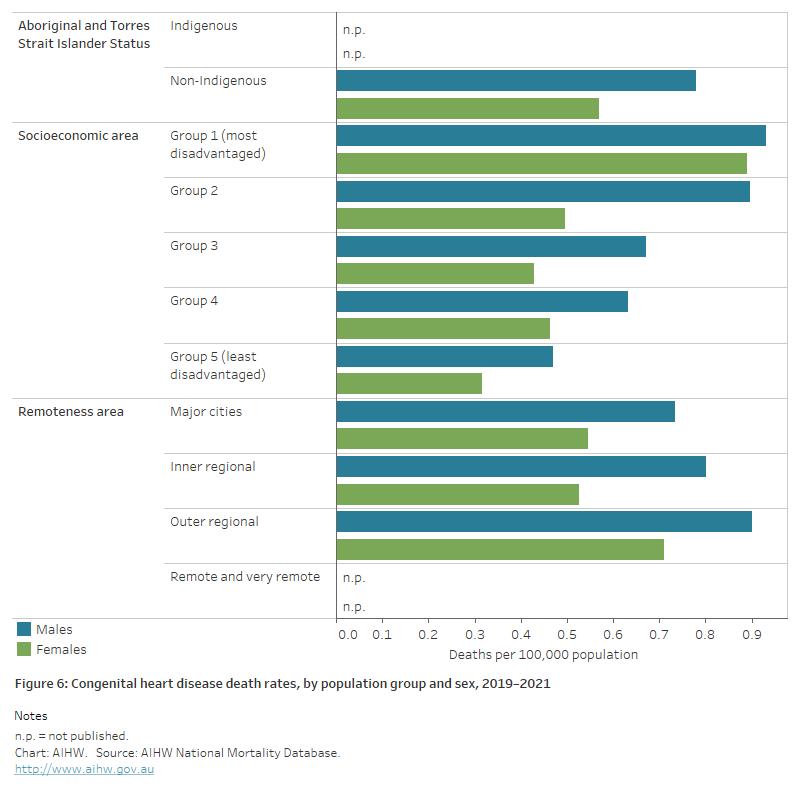
The horizontal bar chart shows in 2019–2021, age-standardised congenital heart disease death rates were similar among Indigenous and non-Indigenous Australians. Rates were slightly higher in the lowest socioeconomic areas, and among people living in Outer regional and Remote and very remote areas.