Hospital care and procedures
Page highlights:
Hospitalisation for all cardiovascular disease
- In 2020–21, there were 600,000 hospitalisations where cardiovascular disease was recorded as the principal diagnosis.
- In 2020–21, cardiovascular hospitalisation rates were around 40% higher among those living in Remote and very remote areas compared with those in Major cities.
- In 2020–21, there were 146,000 coronary angiography procedures reported for patients admitted to hospital – 97,200 (67%) for males and 48,900 (33%) for females.
This section provides an overview of hospital care for all cardiovascular diseases (CVD) in the Australian population. For information on hospitalisations for particular CVD subtypes, refer to the relevant page.
A hospitalisation for CVD may be for medical, surgical, or other acute care, for subacute care (for example rehabilitation) or for non-acute care (for example, maintenance care for a person with limitations due to a cardiovascular condition).
Many patients who are hospitalised with acute cardiovascular events will be cared for in a specialist unit:
- in 2021, there were 103 coronary care units in Australian public hospitals and a further 39 cardiac surgery units (AIHW 2022)
- in 2021, there were 93 specialised stroke units (Stroke Foundation 2021).
Hospitalisation for all cardiovascular disease
 In 2020–21, there were 600,000 hospitalisations where CVD was recorded as the principal diagnosis. This represented 5.1% of all hospitalisations in Australia in 2020–21.
In 2020–21, there were 600,000 hospitalisations where CVD was recorded as the principal diagnosis. This represented 5.1% of all hospitalisations in Australia in 2020–21.
Of these, 530,000 (90%) were for acute care – that is, care in which the intent is to perform surgery, diagnostic or therapeutic procedures in the treatment of illness or injury).
Of these, 542,000 (90%) were for acute care – that is, care in which the intent is to perform surgery, diagnostic or therapeutic procedures in the treatment of illness or injury).
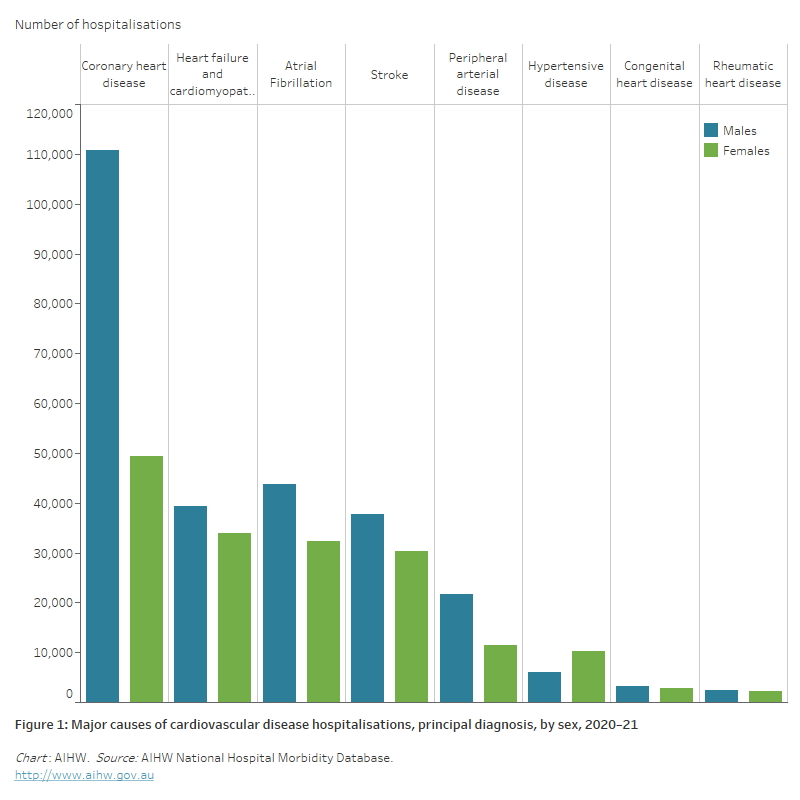
Of all hospitalisations for CVD in 2020–21:
- 27% had a principal diagnosis of coronary heart disease, followed by
- atrial fibrillation (13%)
- heart failure and cardiomyopathy (12%)
- stroke (11%)
- peripheral arterial disease (5.5%)
- hypertensive disease (2.7%)
- rheumatic heart disease (0.8%) (Figure 1).
Figure 1: Major causes of cardiovascular disease hospitalisations, principal diagnosis, by sex, 2020–21
The bar chart shows the number of hospitalisations for selected cardiovascular diseases in 2020–21, ranging from 160,000 for a principal diagnosis of coronary heart disease to 4,600 for rheumatic heart disease.
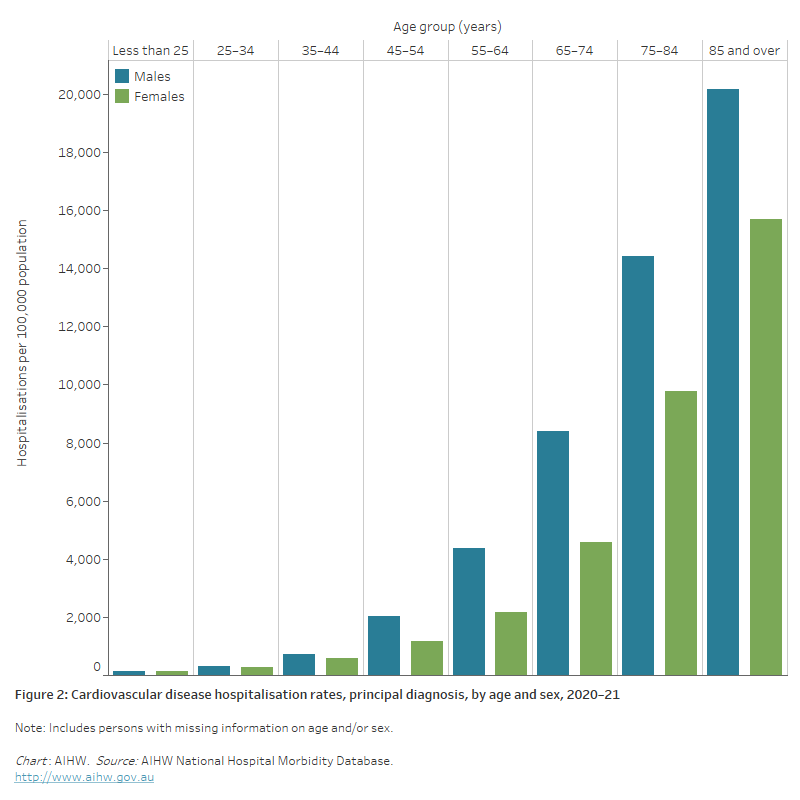
The bar chart shows cardiovascular disease hospitalisation rates by age group in 2020–21. These were highest among men and women aged 85 and over (20,200 and 15,700 per 100,000 population).
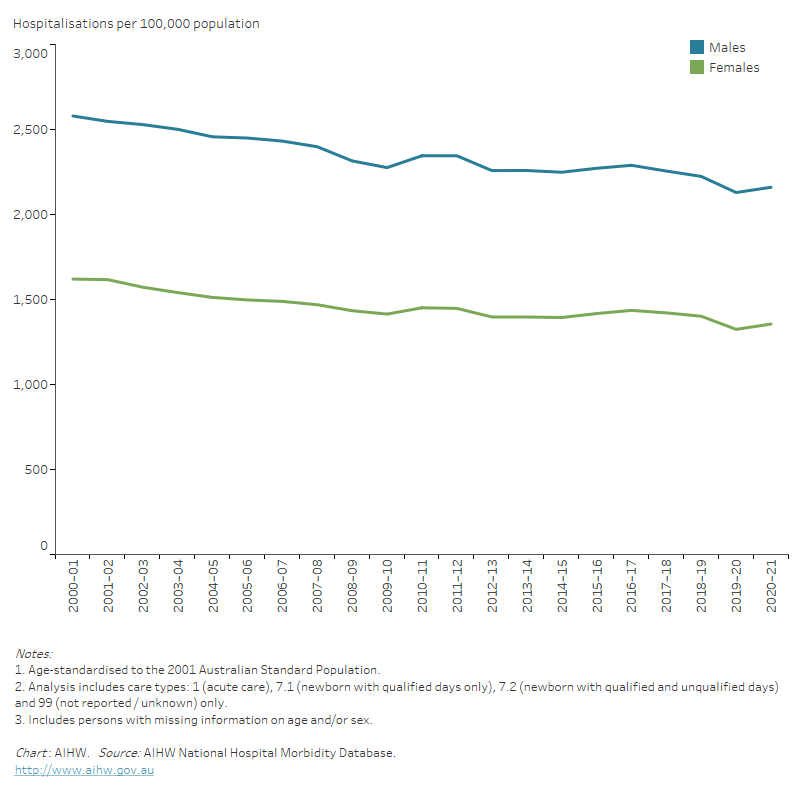
The line chart shows declines in age-standardised rates of male and female acute care CVD hospitalisations between 2000–01 and 2020–21, from 2,570 to 2,160 per 100,000 population for males, and from 1,614 to 1,356 for females.
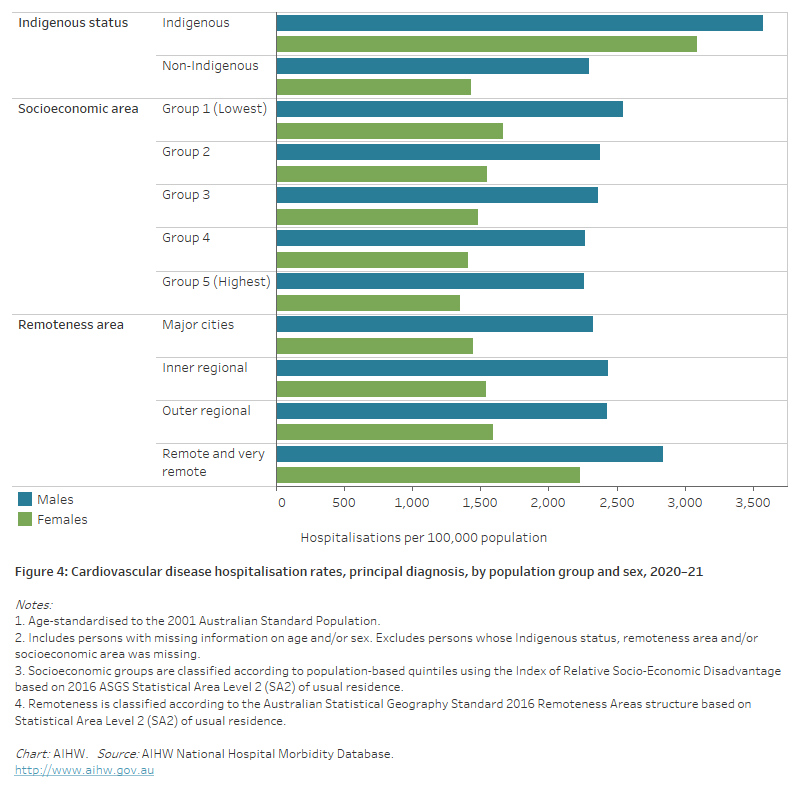
The horizontal bar chart shows that male and female CVD hospitalisation rates in 2020–21 were higher among Indigenous Australians, people living in the lowest socioeconomic areas, and people living in remote and very remote areas.
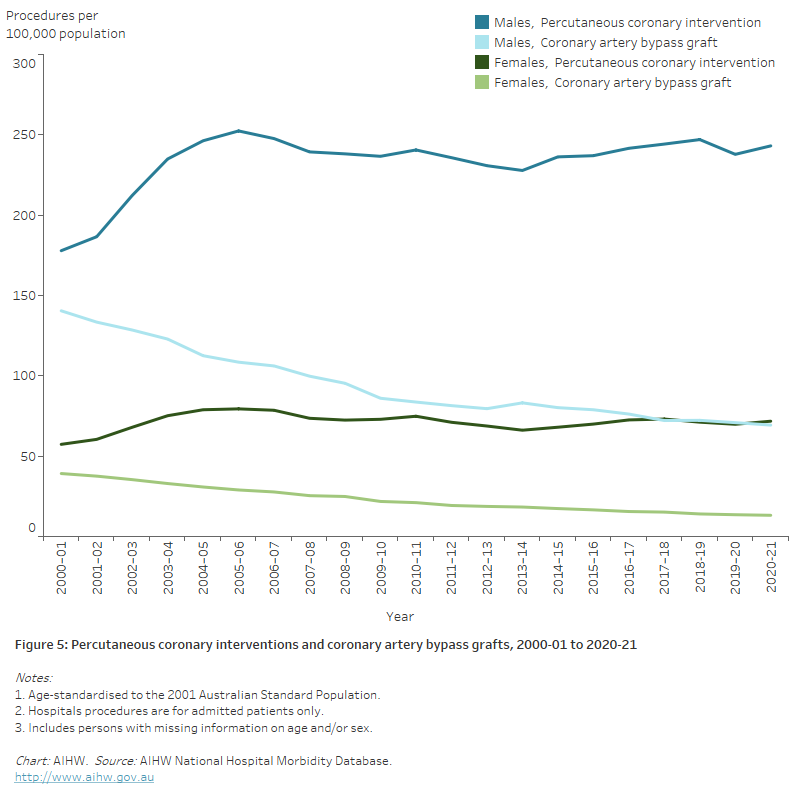
The line chart shows that the number of percutaneous coronary interventions for both males and females increased between 2000–01 and 2020–21, whereas the number of coronary artery bypass grafts declined.