Specialist homelessness services client pathways: analysis insights:
Specialist homelessness services client pathways: Clients with problematic drug or alcohol use in 2015–16
Web article
Last updated:
Topic: Homelessness services
Citation
AIHW
Australian Institute of Health and Welfare (2022) Specialist homelessness services client pathways: Clients with problematic drug or alcohol use in 2015–16, AIHW, Australian Government, accessed 19 April 2024.
APA
Australian Institute of Health and Welfare. (2022). Specialist homelessness services client pathways: Clients with problematic drug or alcohol use in 2015–16. Retrieved from https://pp.aihw.gov.au/reports/homelessness-services/shs-drug-alcohol-use-2015-16
MLA
Specialist homelessness services client pathways: Clients with problematic drug or alcohol use in 2015–16. Australian Institute of Health and Welfare, 07 June 2022, https://pp.aihw.gov.au/reports/homelessness-services/shs-drug-alcohol-use-2015-16
Vancouver
Australian Institute of Health and Welfare. Specialist homelessness services client pathways: Clients with problematic drug or alcohol use in 2015–16 [Internet]. Canberra: Australian Institute of Health and Welfare, 2022 [cited 2024 Apr. 19]. Available from: https://pp.aihw.gov.au/reports/homelessness-services/shs-drug-alcohol-use-2015-16
Harvard
Australian Institute of Health and Welfare (AIHW) 2022, Specialist homelessness services client pathways: Clients with problematic drug or alcohol use in 2015–16, viewed 19 April 2024, https://pp.aihw.gov.au/reports/homelessness-services/shs-drug-alcohol-use-2015-16
Study cohort – Specialist homelessness services: Clients with problematic drug or alcohol use in 2015–16
Introduction
Problematic drug or alcohol use and homelessness are often intertwined. In addition, these clients also often experience other vulnerabilities, such as family and domestic violence and mental health issues which can lead to housing instability and homelessness (see Clients with problematic drug or alcohol use).
Longitudinal analyses have been undertaken for a cohort of clients with problematic drug or alcohol use in 2015–16. These analyses are designed to examine SHS service usage patterns for a cohort of service users that can be tracked for a relatively similar period in the past and into the future.
See Introduction to the SHS longitudinal data for details on the longitudinal analysis undertaken.
The problematic substance use issues (SUB) 2015–16 SHS client cohort was defined as SHS clients that met any of the following conditions in any of the support periods in 2015–16:
- recorded their dwelling type as rehabilitation facility
- required drug or alcohol counselling
- were formally referred to the SHS from an alcohol and drug treatment service
- had been in a rehabilitation facility or institution during the past 12 months
- reported problematic drug, substance or alcohol use as a reason for seeking assistance or the main reason for seeking assistance
- the identification of clients with problematic drug and/or alcohol use may be current or recent; referring to issues at presentation, just prior to receiving support or at least once in the 12 months prior to support.
The above approach is consistent with the definition for clients with problematic drug and/or alcohol use in other AIHW SHS publications such as the 2020–21 SHS annual report (AIHW 2021).
Note that, because the criteria for inclusion in the problematic drug and/or alcohol use cohort includes whether the client had been in a rehabilitation facility or institution during the past 12 months, it is possible that some clients in the cohort do not actually have substance use issues in the defining study period (and do not require services for substance use issues) but had these issues only in the past.
The longitudinal analyses are limited to adult clients (aged 18 and over). This is because the longitudinal analyses focus on pathways for individual clients, whereas children accessing services may need support because of issues that are unrelated to them directly.
A comparison cohort (non-SUB cohort) was also created, comprising clients aged 18 and over who did not meet the criteria for inclusion in the DA cohort. These clients did not meet any of the above conditions in any of the support periods during their defining study period (12 months from the start of their first support period in 2015–16). They were therefore considered to have not had problematic drug and/or alcohol use issues in their defining study period. More information on the how comparison cohorts were derived can be found in the Methodology section.
The longitudinal SHS data for the period 2011–21 were used to (Figure SUB.1):
- examine characteristics of clients with problematic drug and/or alcohol use (termed the SUB cohort) compared with the comparison cohort (the non-SUB cohort)
- examine outcomes for the SUB cohort in terms of historical and future service use.
The retrospective study period for this cohort is the 48 months before the start of the defining study period (that is, the 12 months from the start of their first mental-health related support period in 2015–16). The prospective study period is the 48 months after the end of each client’s 12 month defining study period.
Figure SUB.1: Clients with problematic drug or alcohol use cohort, longitudinal analysis overview
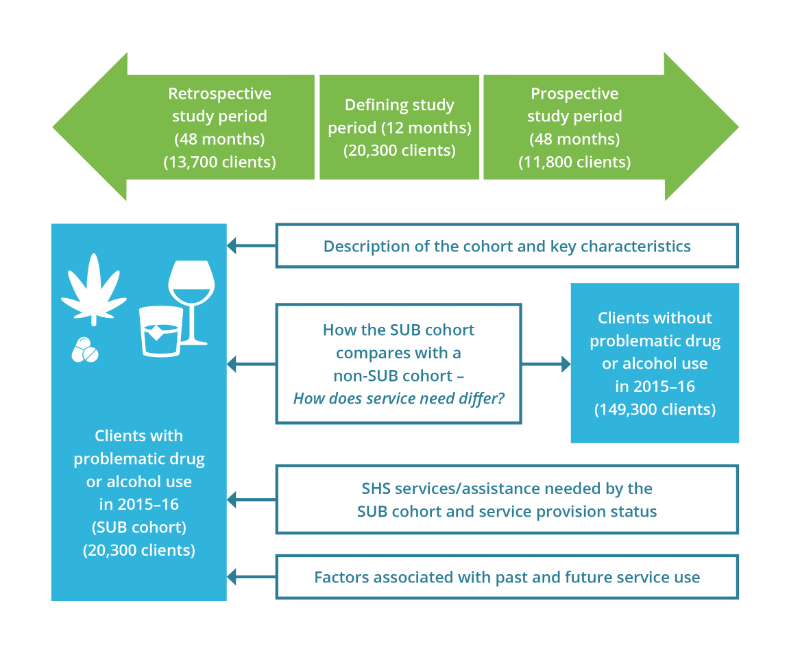
Source: AIHW analysis of SHS longitudinal data 2011–21, Table SUB1516.1.
Key characteristics of the SUB 2015–16 cohort
There were nearly 20,300 clients in the SUB 2015–16 SHS client cohort with the following key characteristics (Table SUB1516.1):
- The mean age of clients was 35 years with over 29% (nearly 6,000 clients) aged 25–34 years and 28% (nearly 5,800 clients) aged 35 to 44 years at the time of their first substance-use-related support period in 2015–16.
- Around 6,300 clients (31%) were Indigenous.
- Nearly 2,300 clients (11%) were born overseas.
- Around 42% of clients (8,500 clients) had only one support period during the defining study period and 36% (7,300) had 3 or more support periods.
- Over 67% had received SHS support previously; that is, nearly 13,700 clients had received SHS support in the 48-month retrospective period that preceded the defining study period. Of these clients, 6,500 clients (32% of the SUB 2015–16 cohort or alternatively 48% of clients that used services in the past) had problematic substance use issues during a historical period of support.
- Over 58% of clients (11,800) continued to receive SHS support into the future; that is, they received support in the 48 months after the 12-month defining study period. Of these clients, nearly 6,400 (31% of the SUB 2015–16 cohort, or alternatively 54% of clients that continued to use services into the future) had problematic substance use issues during a future period of support.
Service engagement profiles
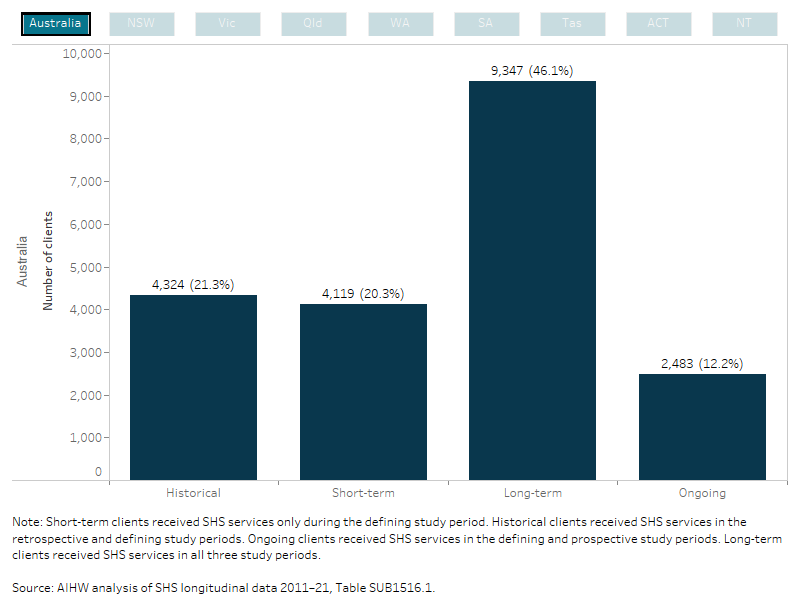
Service use patterns of the SUB cohort over the entire longitudinal period (2011–21) were examined. Almost half (9,300 or 46%) of SUB cohort clients had used SHS support over the 10-year longitudinal period (long-term clients) (Figure SUB.2, Table SUB1516.1).
Figure SUB.2: SUB client cohort 2015–16, service engagement profiles
This interactive bar chart shows service use patterns of the SUB cohort over the entire longitudinal period (2011–21). Support information was combined from the discrete study periods into four service engagement profile groups (historical, short-term, long-term and ongoing). Engagement profiles for all states and territories and Australia can be selected and displayed. Nationally, of the 20,300 clients that made up the study period cohort, almost half (9,300 or 46%) of SUB cohort clients had used SHS support over the 10-year longitudinal period (long-term clients). For ACT clients, 37% were short-term clients and had used SHS support during the defining period only and a small proportion (7%) were ongoing clients (used services in the defining and prospective periods).
This interactive bar chart shows a comparison between the SUB and non- SUB cohorts, in terms of key characteristics and across all study periods (defining, retrospective and prospective). A radio button allows selection for the individual state/territory and Australia. For Australia, the SUB cohort had a similar age profile to the non- SUB cohort, however clients in the SUB cohort were more likely to be male; 55% compared with 34% for the non- SUB cohort. Nearly all clients in the SUB cohort (96%) were not employed (that is, unemployed or not in the labour force) at some time during the defining study period compared with 78% of clients in the non-SUB cohort.

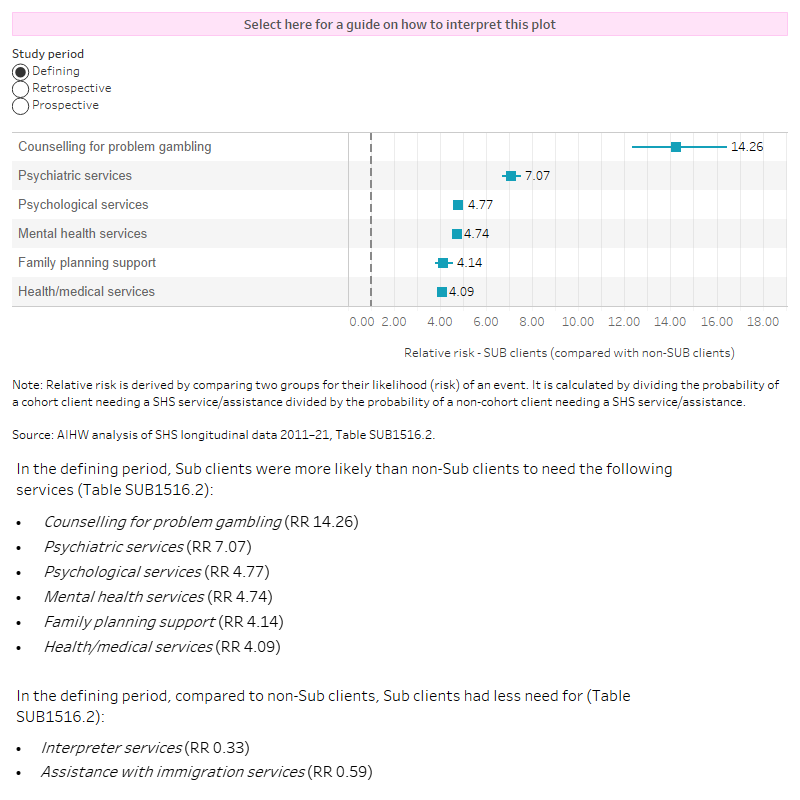
The interactive risk ratio plot shows the differences in service need between SUB and non- SUB clients receiving SHS support in each study period, these associations are presented as relative risks. The top 6 services more likely to be needed by SUB cohort clients compared with non- SUB clients (that is, those with the largest relative risk) have been shown in the figure. A radio button allows selection of the services and relative risks for each of the study periods (defining, retrospective and prospective). Clients with problematic drug or alcohol use were over 14 times more likely to need counselling for problem gambling (relative risk (RR) 14.26) during the 2015–16 defining study period than clients in the non-SUB cohort.
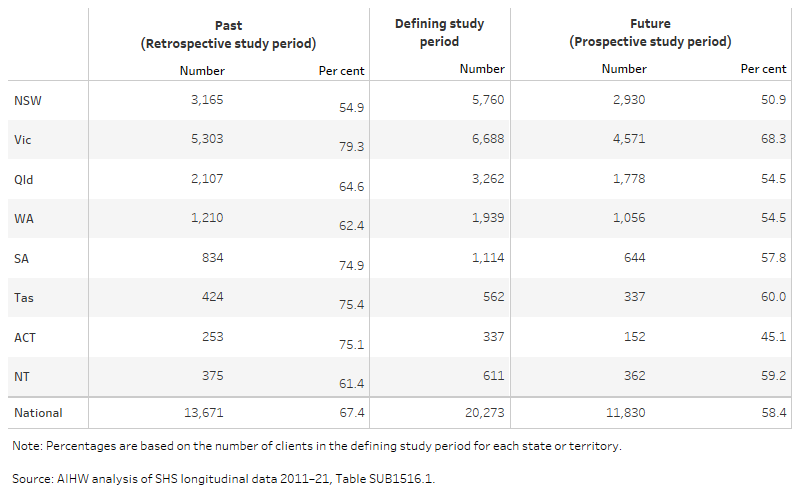
The table image shows the number and per cent of SUB cohort clients within each study period for each state and territory and Australia. One third (33%; 6,700) of clients received their first support period in 2015–16 from agencies located in Victoria, followed by 28% in New South Wales and 16% in Queensland. The proportion of clients that received SHS support in the past ranged from 55% of the cohort in New South Wales to 79% of the cohort in Victoria. The proportion of clients that received SHS support in the future (after the defining study period) ranged from 45% in the ACT to 68% in Victoria.
|
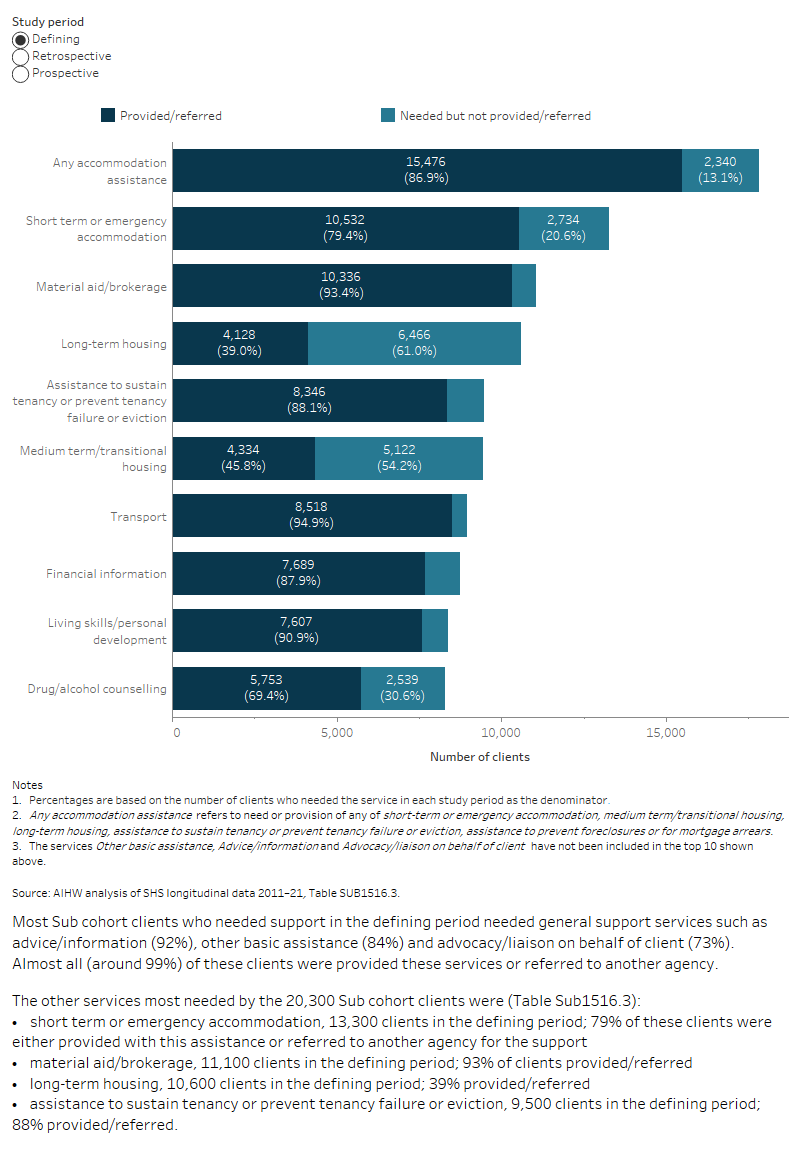
The interactive stacked horizontal bar graph shows the select top 10 services needed and the provision/referral status for the SUB cohort clients (20,300 clients) that used services in the retrospective, defining and prospective study periods. Patterns of service need were generally similar for the 2015–16 SUB cohort across the three study periods. For example, the proportion of clients with a need for accommodation assistance (all forms) was similar and pervasive (around 89%) in all study periods. |
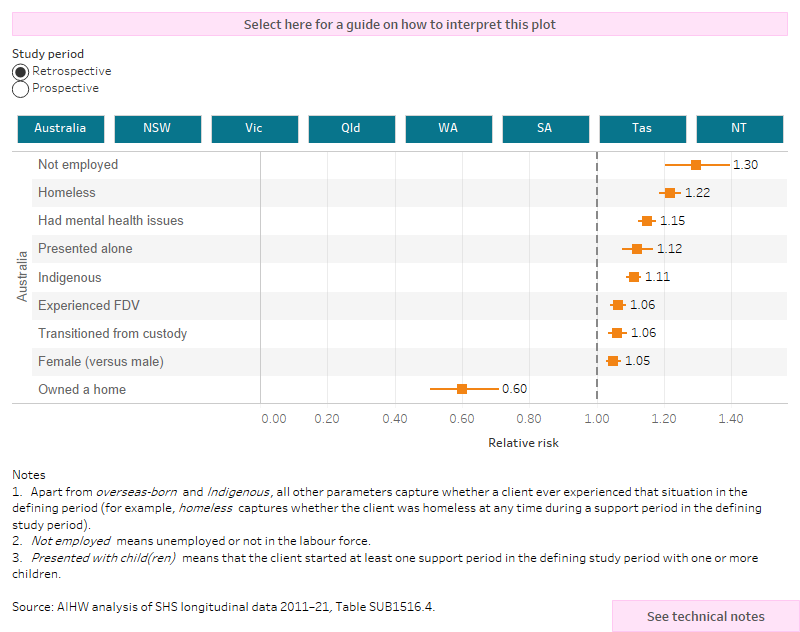
The interactive risk ratio plot shows the characteristics or circumstances that are associated with the SUB cohort clients use of SHS services in the past (retrospective) or future (prospective period), these associations are presented as relative risks. Relative risks for all states and territories and Australia can be selected and displayed. The results show that having owned a home was associated with reduced likelihood of having a history or ongoing use of SHS support, although the associations vary in magnitude within each state or territory. Most other factors were associated with a greater likelihood of past and future SHS support, especially not being employed, having been homeless, having mental health issues.