Injury in Australia:
Choking and suffocation
Web article
Last updated:
Topic: Injury
Part of Injury in Australia
Citation
AIHW
Australian Institute of Health and Welfare (2023) Choking and suffocation, AIHW, Australian Government, accessed 23 April 2024.
APA
Australian Institute of Health and Welfare. (2023). Choking and suffocation. Retrieved from https://pp.aihw.gov.au/reports/injury/choking-and-suffocation
MLA
Choking and suffocation. Australian Institute of Health and Welfare, 06 July 2023, https://pp.aihw.gov.au/reports/injury/choking-and-suffocation
Vancouver
Australian Institute of Health and Welfare. Choking and suffocation [Internet]. Canberra: Australian Institute of Health and Welfare, 2023 [cited 2024 Apr. 23]. Available from: https://pp.aihw.gov.au/reports/injury/choking-and-suffocation
Harvard
Australian Institute of Health and Welfare (AIHW) 2023, Choking and suffocation, viewed 23 April 2024, https://pp.aihw.gov.au/reports/injury/choking-and-suffocation
 1,500 hospitalisations in 2021–22
1,500 hospitalisations in 2021–22
5.6 per 100,000 population
 1,200 deaths in 2020–21
1,200 deaths in 2020–21
4.6 per 100,000 population
For more detail, see Data tables C1–3 and F1–4.
Seasonal differences
Patterns of hospitalisation due to choking and suffocation remain similar across seasons (Figure 2).
Some other causes of injury show seasonal differences – see the interactive display.
Figure 2: Seasonal differences in hospitalisations due to choking and suffocation, 2019–20 to 2021–22
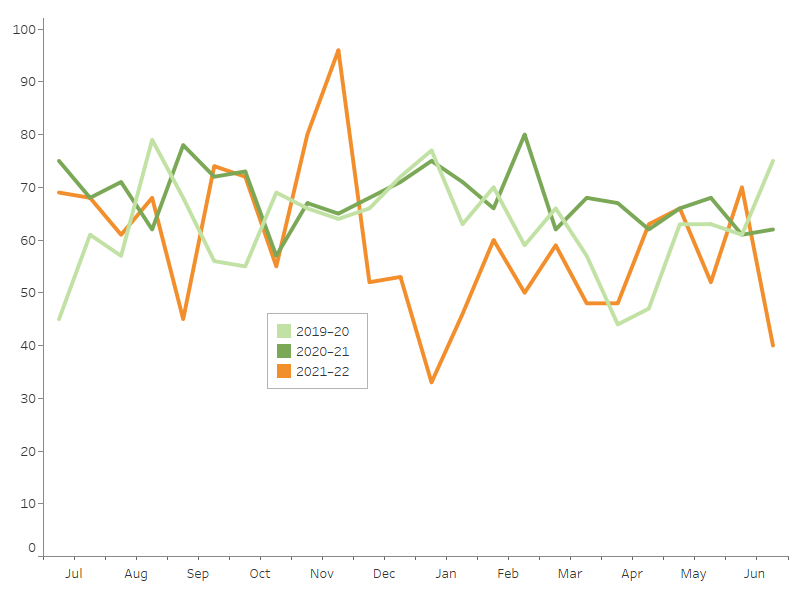
Notes
- Admission counts have been standardised into two 15-day periods per month.
- A scale up factor has been applied to June admissions to account for cases not yet separated.
Source: AIHW National Hospital Morbidity Database.
For more detail, see Data tables C1–3 and F1–4.
Age and sex differences
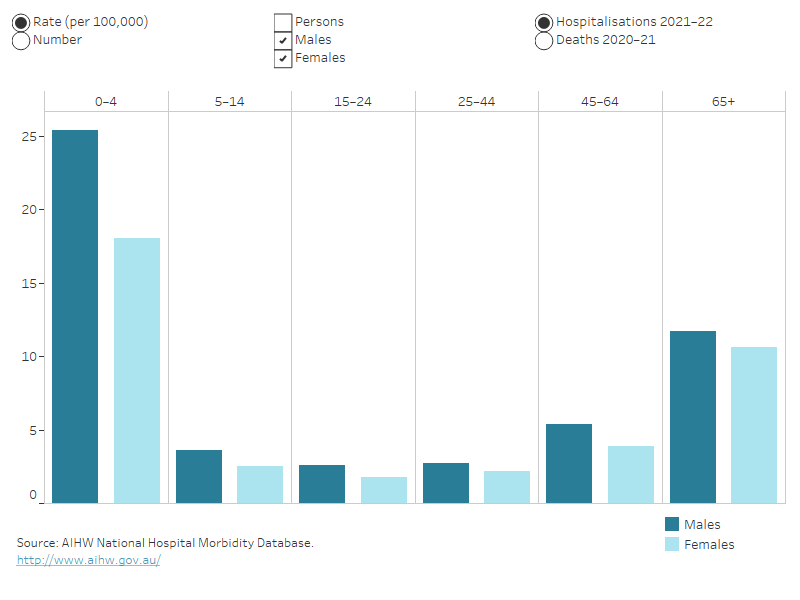
Rates of death due to choking and suffocation were highest for people aged 65 and over, while children aged 0 to 4 had the highest rates of hospitalisation compared with other life-stage age groups.
Of the hospitalisations in 2021–22:
- 33% were for people aged 65 and over
- 23% were for children aged 0–4.
Males were 1.3 times as likely as females to be hospitalised for choking or suffocation in 2021–22.
Of the deaths in 2020–21, 81% were for people aged 65 and over (Figure 3).
Figure 3: Choking and suffocation hospitalisations and deaths, by age group and sex
Column graph representing sex within 6 life-stage age groups. The reader can choose to display either rate per 100,000 population or number, and either hospitalisations or deaths. The default displays rate of hospitalisations for males and females and the reader can also choose to display persons.