Injury in Australia:
Contact with living things
Web article
Last updated:
Topic: Injury
Part of Injury in Australia
Citation
AIHW
Australian Institute of Health and Welfare (2023) Contact with living things, AIHW, Australian Government, accessed 26 April 2024.
APA
Australian Institute of Health and Welfare. (2023). Contact with living things. Retrieved from https://pp.aihw.gov.au/reports/injury/contact-with-living-things
MLA
Contact with living things. Australian Institute of Health and Welfare, 06 July 2023, https://pp.aihw.gov.au/reports/injury/contact-with-living-things
Vancouver
Australian Institute of Health and Welfare. Contact with living things [Internet]. Canberra: Australian Institute of Health and Welfare, 2023 [cited 2024 Apr. 26]. Available from: https://pp.aihw.gov.au/reports/injury/contact-with-living-things
Harvard
Australian Institute of Health and Welfare (AIHW) 2023, Contact with living things, viewed 26 April 2024, https://pp.aihw.gov.au/reports/injury/contact-with-living-things
 28,500 hospitalisations in 2021–22
28,500 hospitalisations in 2021–22
111 per 100,000 population
 27 deaths in 2020–21
27 deaths in 2020–21
0.1 per 100,000 population
Timeline graph for hospitalisations. 3 lines represent the trend for males, persons and females over 10 years. The reader can choose to display rate per 100,000 population or number.
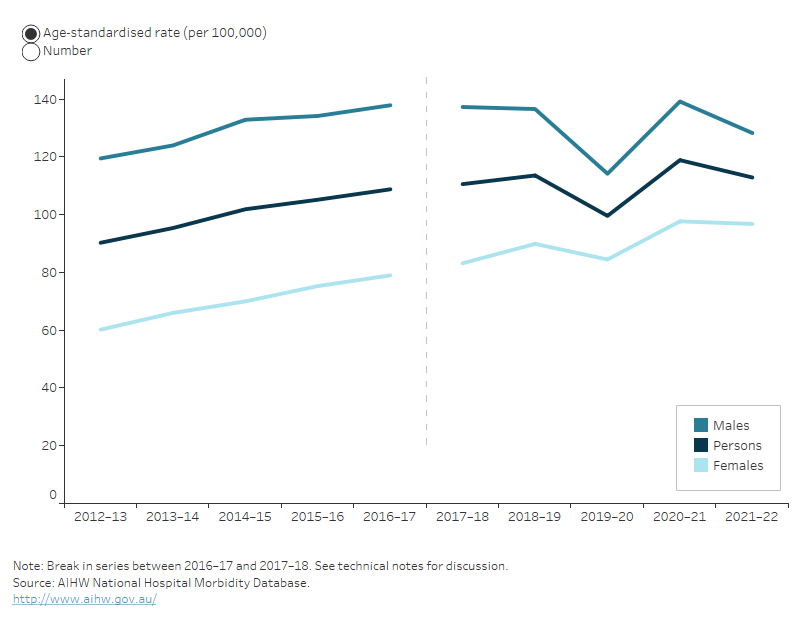
For more detail, see Data tables C1–3 and F1–4.
Seasonal differences
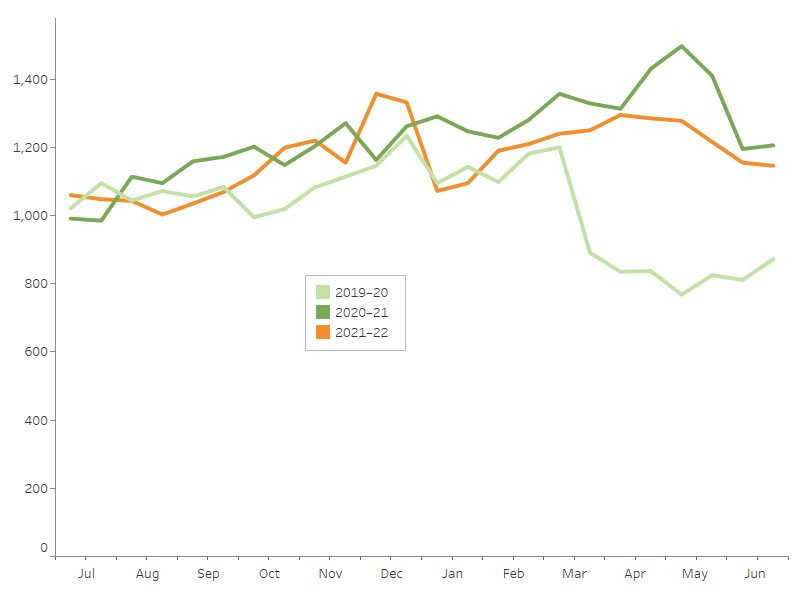
Hospitalisations due to contact with living things display a minor seasonal pattern, with peaks in summer and autumn (Figure 2).
In March 2020, COVID-19 restrictions interrupted the usual activity of Australians, coinciding with a large dip in injury hospitalisations.
The interactive display illustrates other seasonal differences in injury hospitalisations.
Figure 2: Seasonal differences in hospitalisations due to contact with living things, 2019-20 to 2021–22
Notes
1. Admission counts have been standardised into two 15-day periods per month.
2. A scale up factor has been applied to June admissions to account for cases not yet separated.
Source: AIHW National Hospital Morbidity Database.
Age and sex differences
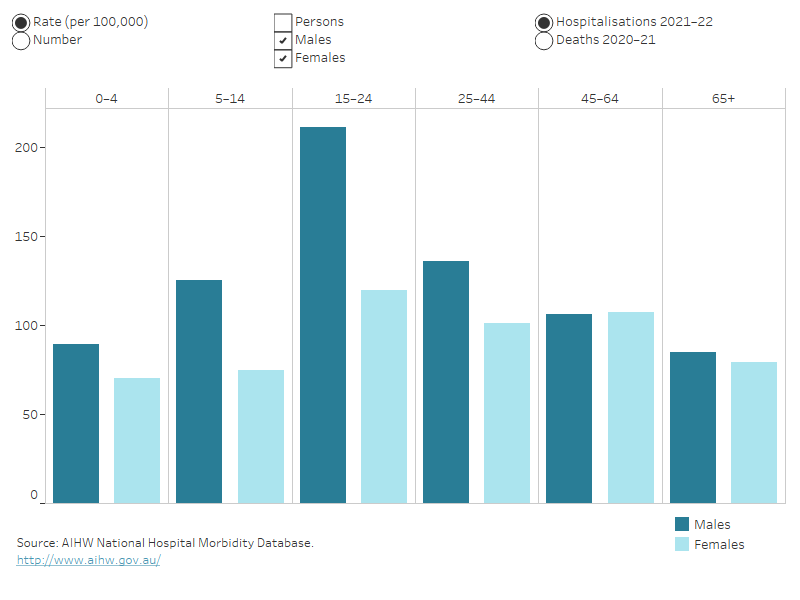
Rates of injuries caused by contact with living things differ by sex and across age groups. In 2021–22:
- 56% of the hospitalisations were for males
- the age-standardised rates of hospitalisation were 130 cases per 100,000 males, and 97 per 100,000 females
- males aged 15–24 had the highest rate of hospitalisation (Figure 3).
Figure 3: Injury hospitalisations and deaths due to contact with living things, by age group and sex, 2021–22
Column graph representing sex within 6 life-stage age groups. The reader can choose to display either rate per 100,000 population or number. The default displays rate of hospitalisations for males and females and the reader can also choose to display persons, and to display deaths.
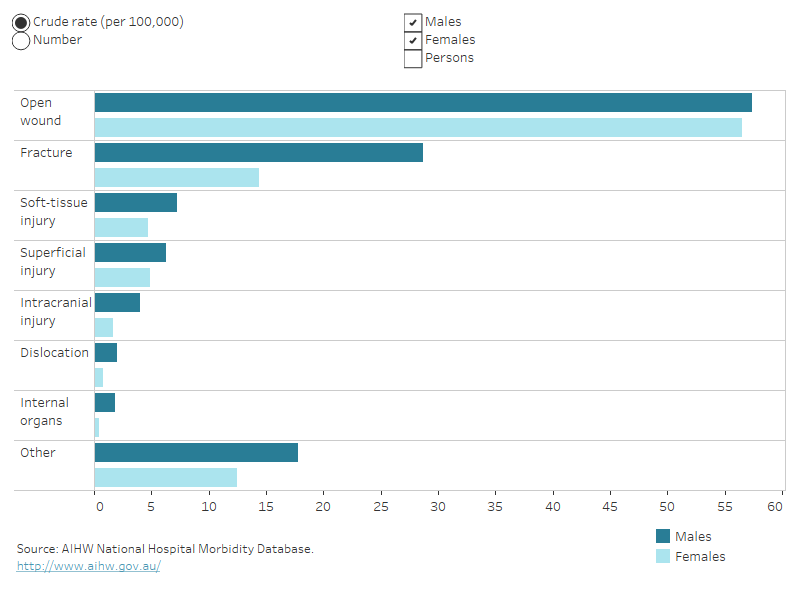
Bar graph showing type of injury sustained by category and by sex. Fracture was the most common for both males and females, followed by open wound. The reader can choose to display either the crude rate per 100,000 population or the number of cases. The default display shows data for males and females, or the reader can choose to display for persons.
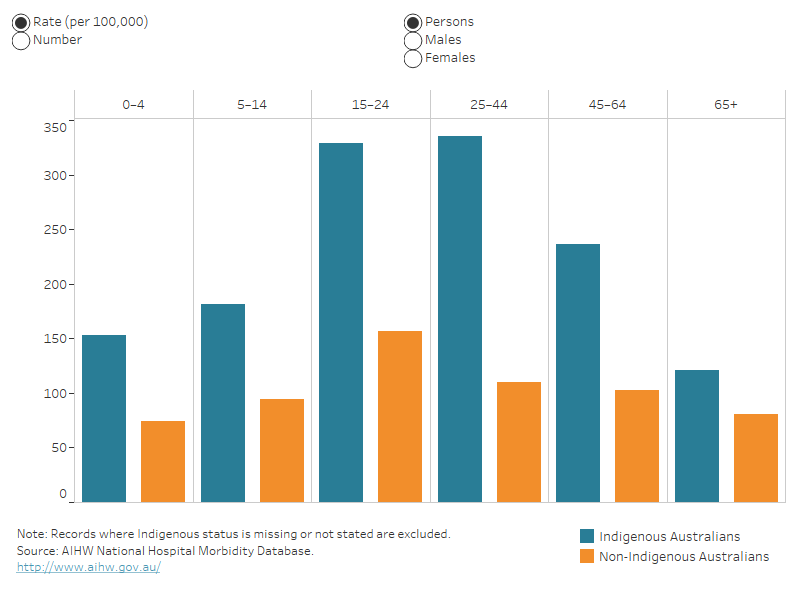
Column graph representing hospitalisation data for Indigenous and non-Indigenous Australians by 6 life-stage age groups. For each age group, the reader can choose to display rate per 100,000 population or number. The reader can also choose to display data for persons, males or females.
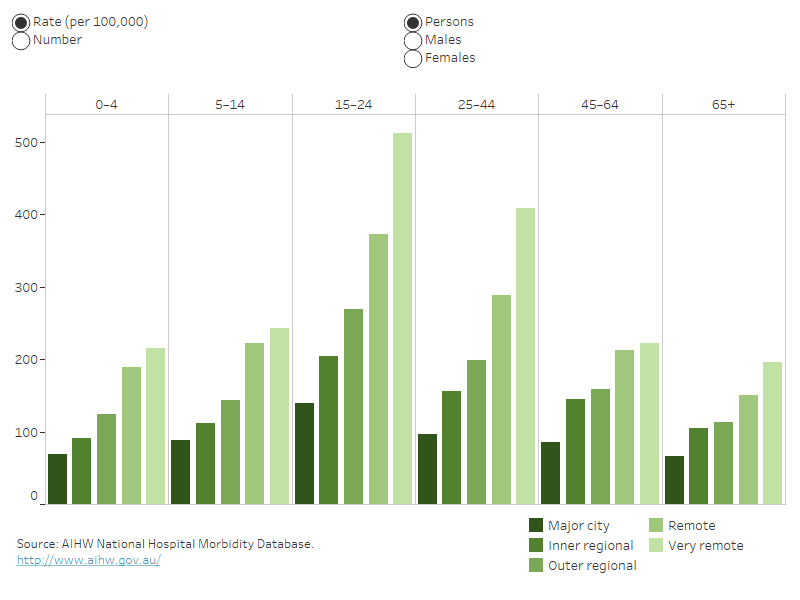
This column graph shows hospitalisations data for each of the 5 remoteness categories by 6 life-stage age groups. For each age group, the reader can choose to display rate per 100,000 population or number. The reader can also choose to display data for persons, males or females.