Patient safety
This section presents data for the patient safety indicators supplied by Australia to the HCQO collection. It compares these data with the HCQO results for other OECD countries, and comments on the comparability of the data provided to the OECD specification (OECD 2021).
Patient safety remains a pressing issue in the delivery of health services, with over 15% of hospital expenditure and activity in OECD countries attributable to treating patients who experienced a safety event, many of which are preventable (OECD 2021). Patient safety indicators screen for events that patients experience during their hospital stays as a result of exposure to the health-care system – either adverse events that cannot be totally avoided or events that should never occur (OECD 2021).
The OECD published all patient safety indicators in OECD.Stat and a selection of patient safety indicators in Health at a glance 2021. Australia submitted results for all 7 patient safety indicators in the data collection:
- Retained surgical item or unretrieved device fragment
- Post-operative wound dehiscence
- Post-operative pulmonary embolism – hip and knee replacement discharges
- Post-operative deep vein thrombosis – hip and knee replacement discharges
- Post-operative sepsis – abdominal discharges
- Obstetric trauma after vaginal delivery with instrument
- Obstetric trauma after vaginal delivery without instrument.
The indicator definitions can be viewed here: ![]() patient safety indicator definitions
patient safety indicator definitions
PS1.1 presents OECD countries with data available for retained surgical item or unretrieved device fragment indicator in 2018, which shows Australia had the highest rate. PS1.2 presents Australia’s 10-year trend for this indicator, which shows a fluctuating trend over time.

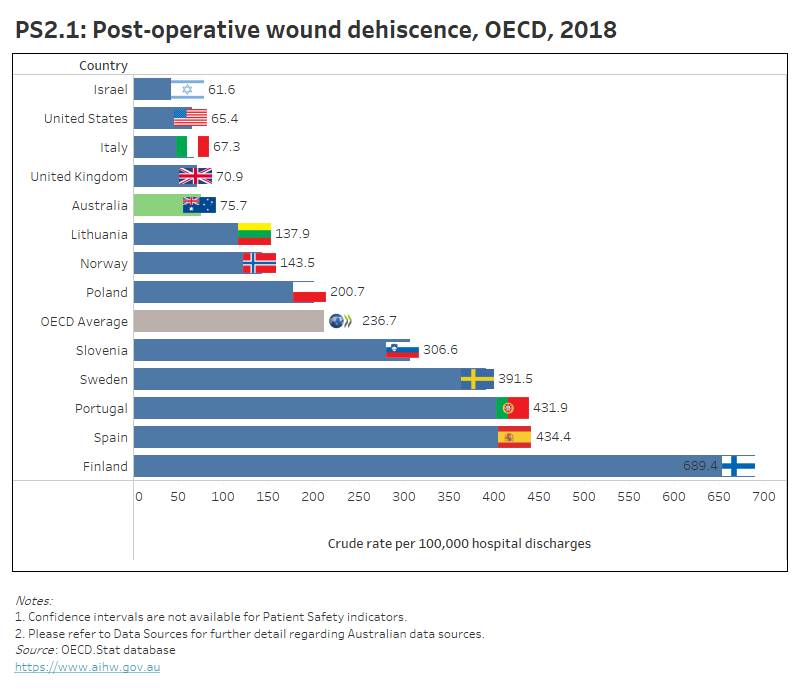
PS2.1 presents OECD countries with data available for post-operative wound dehiscence indicator in 2018, which shows Australia had a lower rate than the OECD average. PS2.2 presents Australia’s 10-year trend for this indicator, which shows a decrease since 2009.
PS3.1 presents OECD countries with data available for post-operative PE in hip and knee replacement discharges indicator in 2018, which shows Australia had the highest rate. PS3.2 presents Australia’s 10-year trend for this indicator, which shows a fluctuating trend over time.

PS4.1 presents OECD countries with data available for post-operative DVT in hip and knee replacement discharges indicator in 2018, which shows Australia had the highest rate. PS4.2 presents Australia’s 10-year trend for this indicator, which shows a decrease since 2010.

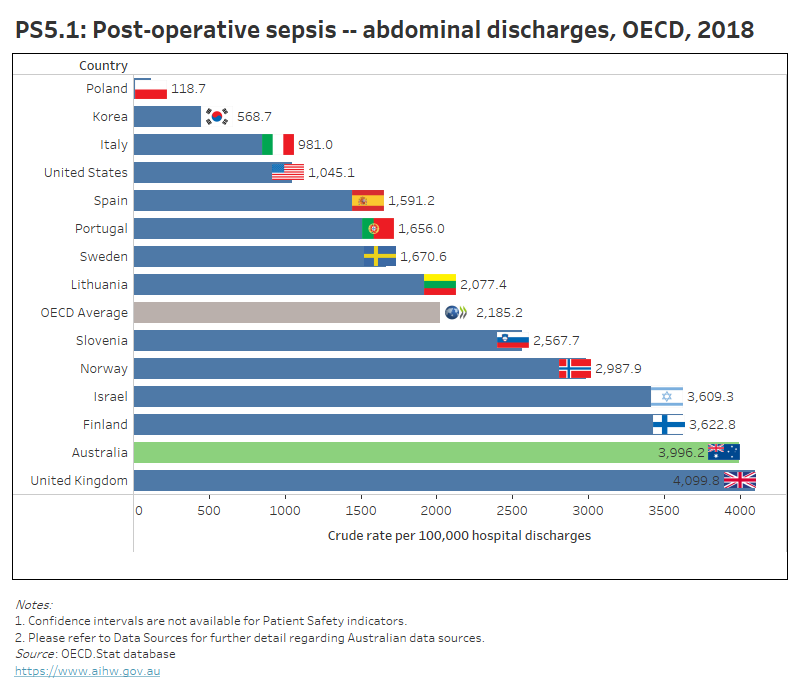
PS5.1 presents OECD countries with data available for post-operative sepsis in abdominal discharges in 2018, which shows Australia had the 2nd highest rate. PS5.2 presents Australia’s 10-year trend for this indicator, which shows an increase since 2011.
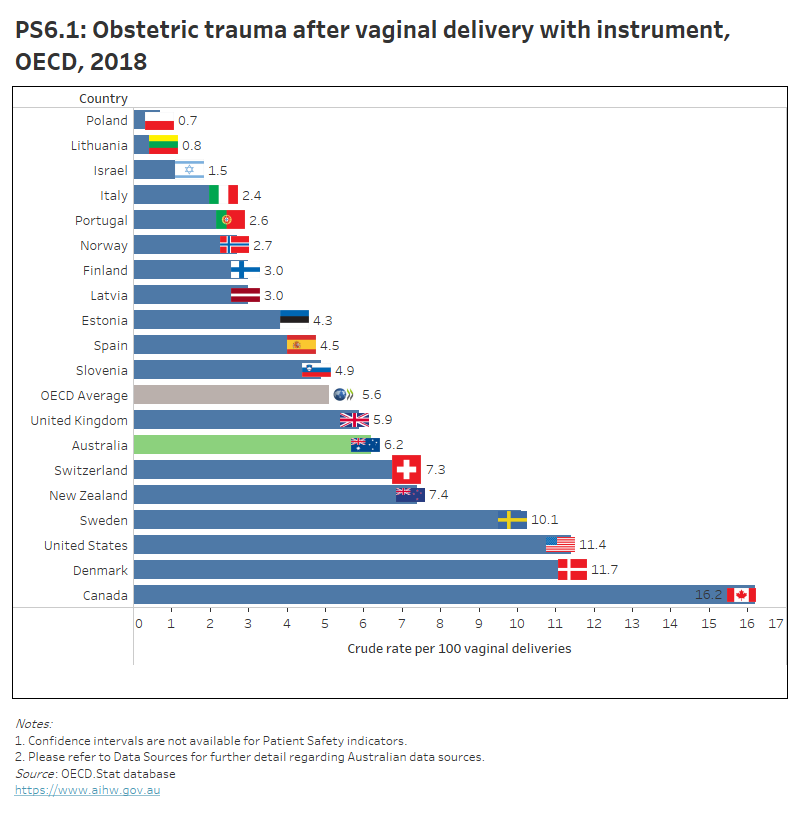
PS6.1 presents OECD countries with data available for obstetric trauma with instrument indicator in 2018, which shows Australia had a higher rate than the OECD average. PS6.2 presents Australia’s 10-year trend for this indicator, which shows a gradual decrease since 2010.
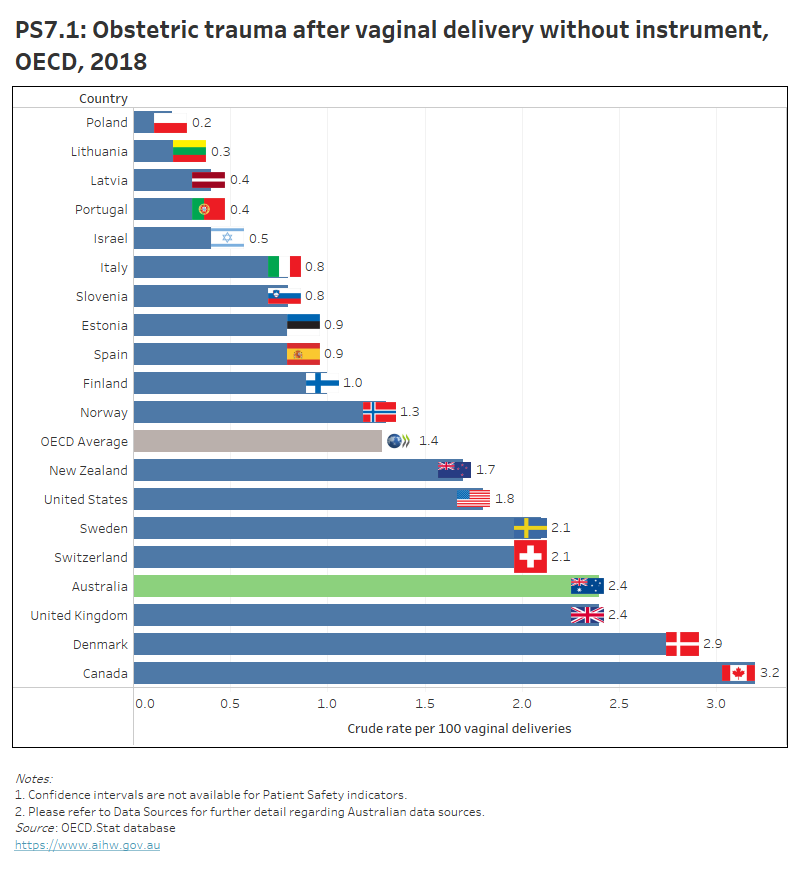
PS7.1 presents OECD countries with data available for obstetric trauma without instrument indicator in 2018, which shows Australia had the 3rd highest rate. PS7.2 presents Australia’s 10-year trend for this indicator, which shows a stable trend since 2010.