How healthy are Australia’s males?
A person’s health status is a general measure combining physical, social, emotional and mental health and wellbeing. A person’s overall level of health can be measured through:
- self-assessment
- burden of disease analysis
- the health impact of disease
- injury in a population
- presence of chronic conditions and comorbidities
- mental health
- sexual health
- life expectancy.
Self-assessed health status reflects a person’s perception of their own health at a particular point in time; it can give a broad picture of the population’s overall health (ABS 2018d).
In 2020–21, 58% of males rated their health as excellent of very good. The proportion of males who rated their health as excellent or very good varies by age group. Eight in 10 (80%) of males aged 15–24 rated their health as excellent or very good compared with 36% of males aged 75 and over in 2020–21 (ABS 2022d).
Burden of disease quantifies the health impact of disease on a population in a given year – both from dying early and from living with disease or injury. The summary measure disability-adjusted life years (DALY) measures the years of healthy life lost from both premature death (fatal burden) and ill health (non-fatal burden).
In 2022 (AIHW 2022d):
- Australian males experienced a greater share of ill health and death (53%) than females (47%)
- after adjusting for age, males experience 1.2 times the rate of total burden and 1.6 times the rate of fatal burden of females, while rates of non-fatal burden are similar
- Australian males lost more healthy years of life from dying prematurely (54%) than from living with disease and injury (46%)
- the highest proportion of ill health and death for males was due to these top 5 disease groups: cancer (19%), cardiovascular diseases (14%), mental health conditions/substance use disorders (11%), injuries (11%), and musculoskeletal conditions (11%) (Figure 1)
- males experienced a greater share than females of ill health and death from some disease groups including injuries (70%), kidney & urinary diseases (62%), cardiovascular diseases (60%), endocrine disorders (mostly diabetes) (58%), infant & congenital conditions (58%) and cancer (56%).
Figure 1: Leading causes of ill health and death (% DALY) by disease group, males, 2022
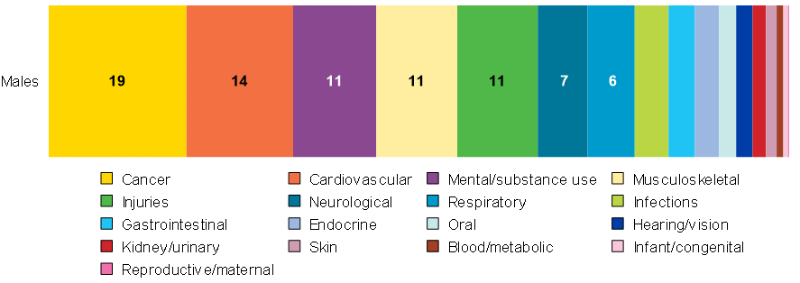
Notes:
DALY = Disability Adjusted Life-Year. This is a measure of healthy life lost, either through premature death or living with disability due to ill health. It is the basic unit used to measure the burden of a disease.
Source: AIHW analysis of AIHW 2022d
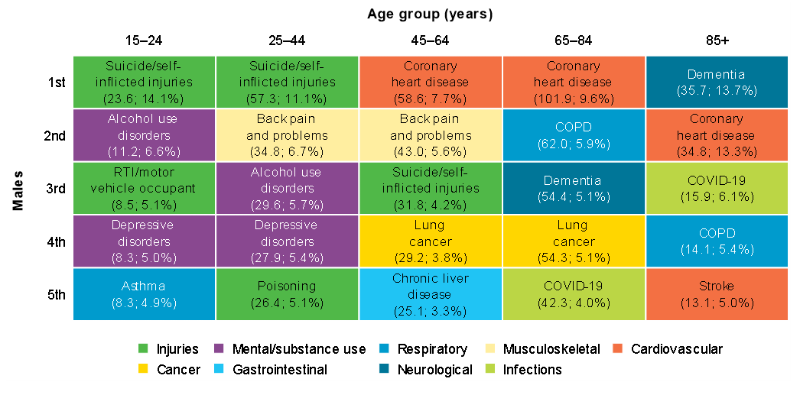
Ill health and death vary across age groups for males. Suicide and self-inflicted injuries were the leading cause of total burden for males aged 15–44. Alcohol use disorders was ranked second for total burden among males aged 15–24, with back pain second among those aged 25–44. Coronary heart disease was the leading cause of burden among males aged 45–84, and second for those aged 65 and over. COVID-19 features for the first time in the top 5 leading causes for males aged over 65 (Figure 2) (AIHW 2022d).
For more information see Australian Burden of Disease Study 2022.
Figure 2: Leading causes of ill health and death (DALY'000; proportion %) among males aged 15 and over, 2022
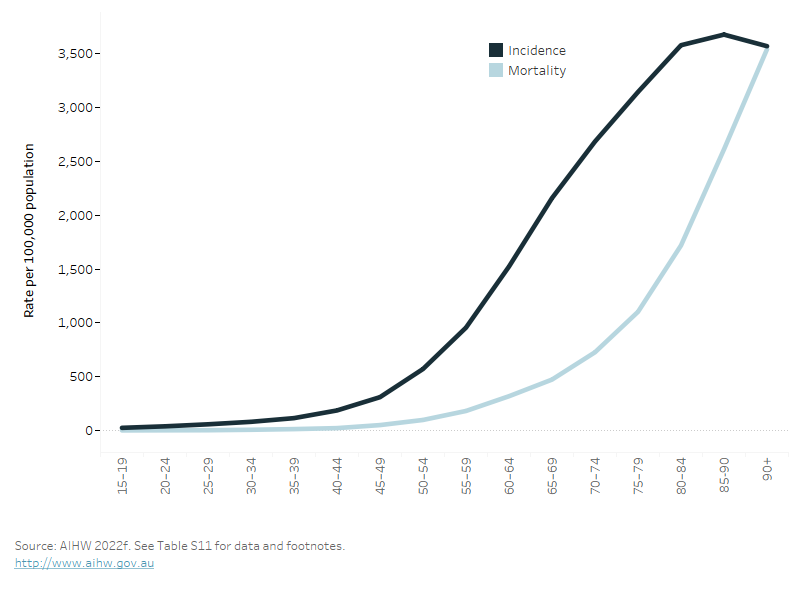
The figure shows that the incidence of all cancers increases with age, as does the associated mortality. However, mortality is delayed due to the period of living with cancer.
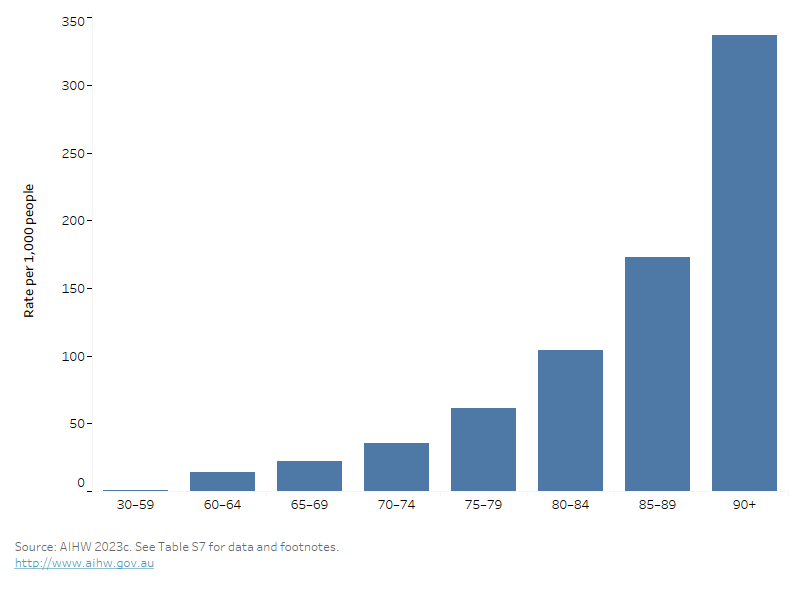
This bar chart shows the rate of dementia across age groups, with the prevalence increasing with age and highest in those aged 90 and over.
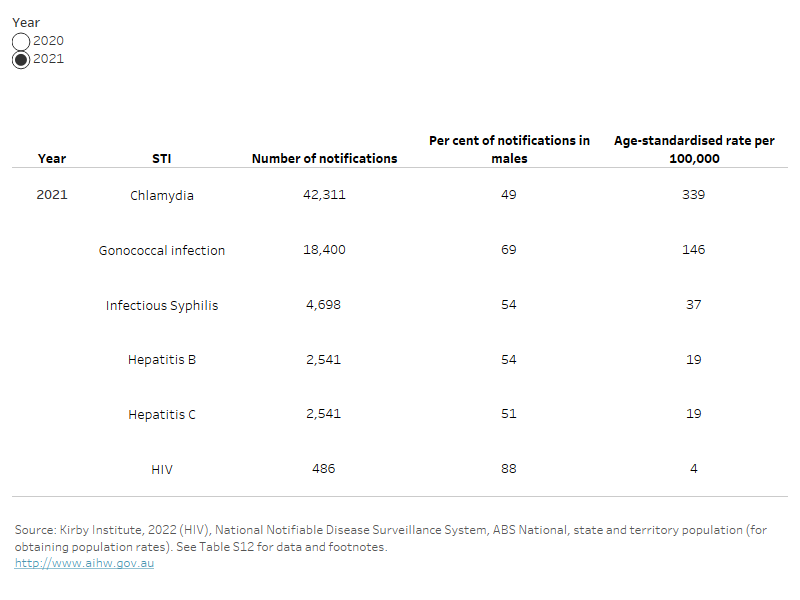
This table shows the number of notifications, per cent of total cases, and age-standardised rates of notifications for chlamydia, gonococcal infection, syphilis, hepatitis b and c for the years 2020 to 2022. For HIV, only 2020 and 2021 data are available.
The line graph shows the notification rates for chlamydia, gonorrhoea and syphilis across the years, from 2012 to 2022. It shows an increase in rates for all three infections.
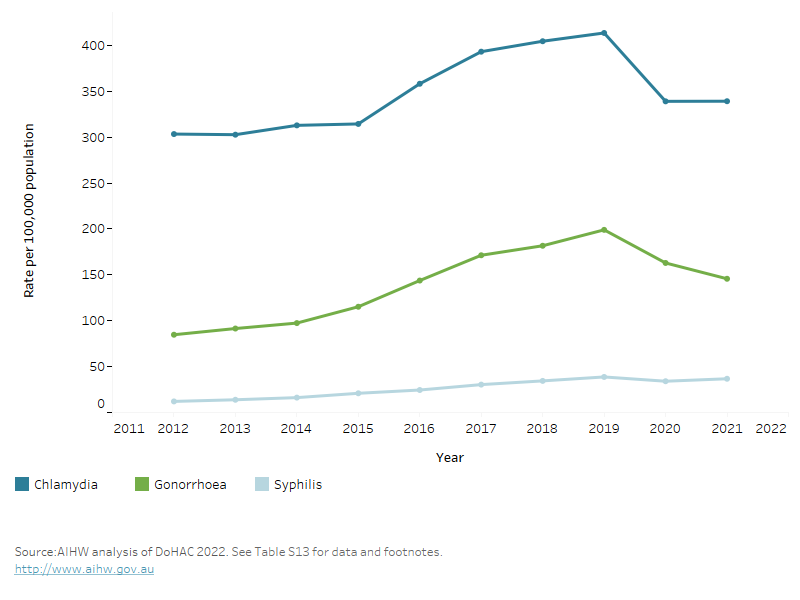
For more information, see HIV, viral hepatitis and sexually transmissible infections in Australia: Annual surveillance report 2022, and the Department of Health and Aged Care National Notifiable Disease Surveillance System.
For more information on male sexual health, see the Healthy Male organisation website Healthy Male Australia: Generations of healthy Australian men.
Life expectancy and mortality
Life expectancy is expressed as either the number of years a newborn baby is expected to live, or the expected years of life remaining for a person at a given age.
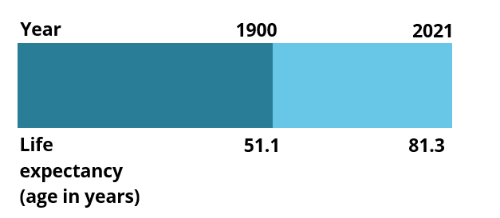
Source: AIHW 2022h
Life expectancy at birth in Australia has improved dramatically in the last century, and males born in 2019–2021 can expect to live 30 years longer than males born in 1891–1900 (ABS 2022h):
- Males born in Australia in 2019–2021 can expect to live to the age of 81.3 years on average (an increase of 1.6 years in the past 10 years) (ABS 2022f).
- International comparisons of life expectancy at birth for males in 2021 indicate that Australian males have the sixth highest life expectancy in the world (81.2 years). Switzerland is ranked first with 81.9 years (OECD 2021).
For more information see: Deaths in Australia: Life expectancy.
Health Adjusted Life Expectancy
Health Adjusted Life Expectancy (HALE) reflects the length of time an individual at a specific age could, on average, expect to live in full health. It can be measured at any age but is typically reported:
- from birth
- at age 65, describing health in an ageing population.
Life expectancy for males born in 2022 is 81.2 years, while the average number of healthy years for these babies is 71.6 years (AIHW 2022d). The difference between life expectancy and HALE (that is, the time expected in less than full health) is 9.6 years. This means that males can expect to spend 88% of their lives in full health (AIHW 2022d).
Males born in 2022 are expected, on average, to live 4.1 years less than females, and are expected to have 2.5 less years of healthy life than females (AIHW 2022d).
Life expectancy in 2022 for males aged 65 was 20.3 years; that is, they could expect to live to the age of 85. At age 65, males could expect on average 15.3 healthy years of life and 5.0 years in less than full health (AIHW 2022d).
Between 2003 and 2022, life expectancy and HALE at birth increased for males. Males gained 3.1 years in life expectancy (from 78.1 years in 2003 to 81.2 in 2022) and 2.2 years in HALE (from 69.4 to 71.6 years) (AIHW 2022d).
For more information see: Australian Burden of Disease Study 2022.
Mortality
Looking at how many people die and what caused their deaths can provide vital information about the health of a population. Patterns and trends in deaths can help explain differences and changes in the health of a population (AIHW 2022h).
Causes of death can be used to:
- assess the success of interventions to improve disease outcomes
- signal changes in community health status and disease processes
- highlight inequalities in health status between population groups.
In 2021, around 89,400 Australian males died. The median age at death was 79.6 years and the leading cause of death was coronary heart disease (12%), followed by dementia including Alzheimer’s disease (6.3%), and lung cancer (5.6%) (Figure 6). The leading causes of death varied by age group (Figure 7) (AIHW 2021a).
The median age at death for males also varies by population group:
- It decreases from 80 years old in Major cities to 66 in Very remote areas (AIHW 2022k).
- It decreases from 81 years in the highest socioeconomic areas, to 77 in the lowest socioeconomic areas (AIHW 2022l).
For more information see Deaths in Australia: Life expectancy.
Figure 6: Leading causes of death, males of all ages, 2021
This horizontal bar chart shows the leading causes of death in males. Leading causes of death include coronary heart disease, dementia including Alzheimer's disease and lung cancer.

This horizontal bar chart shows the top three causes of death in rank order, and the changes with increasing age groups. Suicide affects younger age groups while coronary heart disease is ranked as the leading cause of death for those aged 45 and over.
