Risk factors
Risk factors
Rates of health risk factors, such as smoking and obesity, are higher for Aboriginal and Torres Strait Islander peoples (AIHW 2020a).
Smoking during pregnancy
Smoking during pregnancy is a preventable risk factor for pregnancy complications and is associated with poorer perinatal outcomes, including low birthweight, being small for gestational age, pre-term birth and perinatal death (AIHW 2022a).
Smoking is associated with socioeconomic disadvantage – with the prevalence of smoking increasing with levels of socioeconomic disadvantage (Bonevski and Baker 2012). Evidence suggests that action at both the system level and the individual level can reduce smoking rates (Bonevski and Baker 2012).
Aboriginal and Torres Strait Islander peoples are more likely to smoke than non-Indigenous Australians (AIHW 2020a). The vast majority of Aboriginal and Torres Strait Islander people who smoke want to quit or wish they had never started smoking (Kennedy and Maddox 2022).
Some pregnant Aboriginal and Torres Strait Islander women have reported difficulties with stopping smoking due to their social environment and daily stressors and a lack of culturally sensitive support and information (Passey et al. 2012; Tzelepis et al. 2017).
This report shows that Aboriginal and Torres Strait Islander females who gave birth and smoked at any time during their pregnancy were more likely than those who did not smoke, to give birth to a baby who was born pre-term, of low birthweight or small for gestational age (for more information on the effect of maternal smoking see Baby outcomes).
The National Perinatal Data Collection collects information on self-reported smoking status at 3 time points – at any time during pregnancy, in the first 20 weeks of pregnancy and after 20 weeks of pregnancy.
In 2020:
- 43% of Aboriginal and Torres Strait Islander females who gave birth reported having smoked at any time during their pregnancy
- 42% reported having smoked in the first 20 weeks of pregnancy
- 38% reported having smoked after 20 weeks of pregnancy
In comparison, among non-Indigenous females who gave birth 7.5% smoked at any time during pregnancy, 7.1% smoked in the first 20 weeks of pregnancy and 5.4% smoked after 20 weeks of pregnancy.
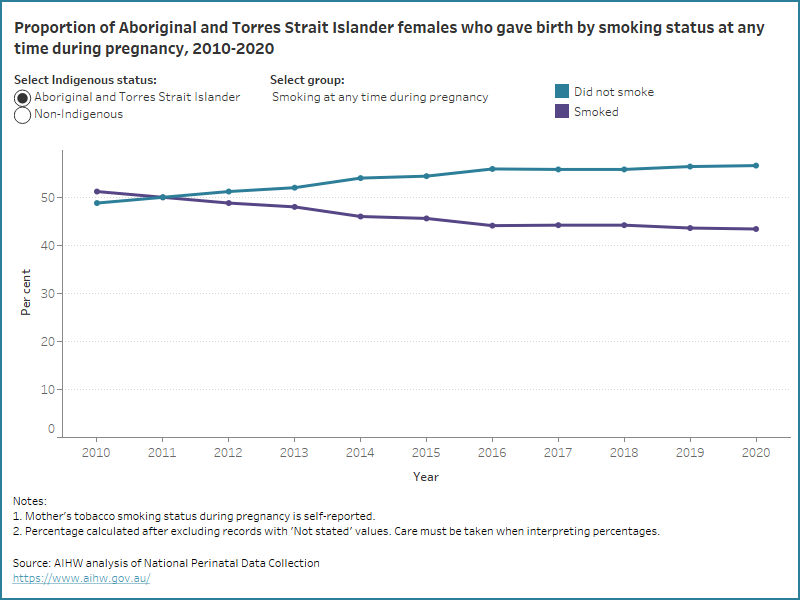
Over time, the proportion of Aboriginal and Torres Strait Islander mothers who smoked at any time during pregnancy has decreased (from 51% in 2010 to 43% in 2020), as has the proportion who smoked in the first 20 weeks of pregnancy (from 50% in 2011 to 42% in 2020) and after 20 weeks of pregnancy (from 45% in 2011 to 38% in 2020).
Some Aboriginal and Torres Strait Islander women who were participants in the community-led Which Way? Smoking Cessation Study reported that they would prefer smoking cessation support programs that were delivered in groups, face to face at an Aboriginal health service and by Aboriginal Health Workers (Kennedy and Maddox 2022). One example of a smoking cessation program which uses community level population health promotion activities is the Tackling Indigenous Smoking program (TISRIC 2020).
Some Aboriginal and Torres Strait Islander mothers may smoke before knowing they are pregnant and stop once they find out they are pregnant. In 2020, 13% of Aboriginal and Torres Strait Islander mothers who reported having smoked in the first 20 weeks of pregnancy did not continue to smoke after 20 weeks of pregnancy.
The data visualisation below shows the proportion of Aboriginal and Torres Strait Islander and non-Indigenous females who gave birth by smoking status at any time during pregnancy from 2010, and smoking status in the first 20 weeks of pregnancy or after 20 weeks of pregnancy from 2011.
Figure 1: Proportion of Aboriginal and Torres Strait Islander and non-Indigenous females who gave birth by smoking status from 2010 to 2020
Line graph of smoking status by Indigenous status. Aboriginal and Torres Strait Islander mothers who did not smoke increased.
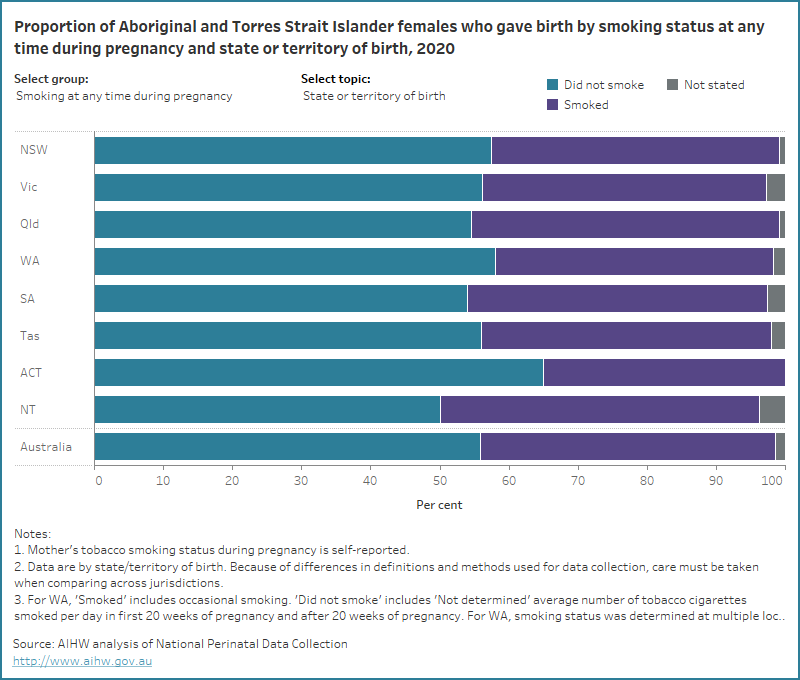
Bar chart for smoking status by selected topics. 56% of Aboriginal and Torres Strait Islander mothers did not smoke at any time during pregnancy.
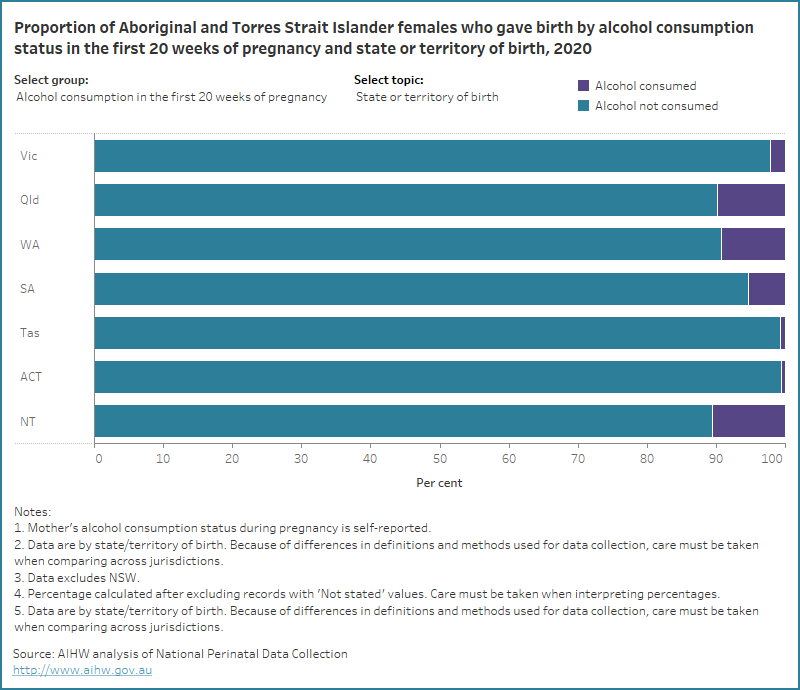
Bar chart for alcohol consumption by selected topics. Most Aboriginal and Torres Strait Islander mothers did not consume alcohol in the first 20 weeks of pregnancy.