Technical notes
On this page
Differences in age structures among ADF service status populations
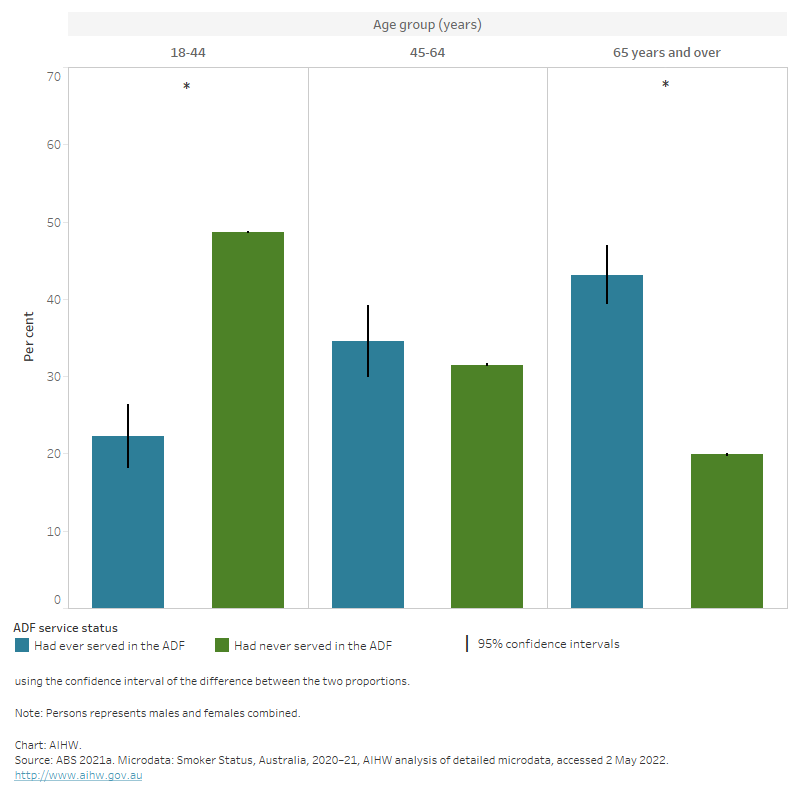
Data from the Smoker Status, Australia 2020–21 data set indicated that those who had ever served in the ADF were typically older than those who had never served (Figure 9). While comparisons can be inferred from the information provided in this report, some differences between persons who had and had not served in the ADF are likely to be confounded by this older age structure of the ADF population. Due to small samples sizes in the Pooled Smoking data set, the counts did not satisfy the minimum data quality requirements for conducting age-standardisation. As such, any comparisons made in this report should be used as a guide only.
Figure 9: Age distribution of persons by ADF service status, 2020–21
The bar chart shows that those who had ever served in the ADF were typically older than those who had never served.
Why does the COVID-19 pandemic matter when measuring veteran smoking?
The COVID-19 pandemic has affected daily life through restrictions on people’s movements and interactions, and has changed how Australians live and work. In particular, the COVID-19 pandemic is suspected to have changed patterns of smoking behaviour globally (Vaneckova et al. 2021; Yang and Ma 2021).
It is important to consider the COVID-19 pandemic as a possible confounding factor when interpreting findings in this report. For example, COVID-19 related lockdowns and restrictions may have reduced access to tobacco products, leading to a reduction in smoking frequency among Australians. Because COVID-19 is a respiratory disease, and smoking is harmful to the respiratory system, smokers may also worry more about becoming seriously ill from a Coronavirus infection, motivating some to reduce or quit smoking (Quit 2022). Alternatively, experiencing the COVID-19 pandemic can evoke negative emotions and increase stress, which may lead to an increase in tobacco consumption (Yang and Ma 2021).
Prior to the COVID-19 pandemic, smoking habits were on the decline. The proportion of adults who have never smoked increased from 49% in 2007–08 to 56% in 2017–18. Since 1995, the proportion of adults who are daily smokers has decreased from 24% to 14% in 2017–18 (ABS 2018).
Due to limitations with how the data was collected during the COVID pandemic, the Smoker Status, Australia 2020–21 data set is considered a break in series, and reflects the specific time point only (ABS 2021b). As such, comparisons to previous smoking data are not recommended.
For more information, see Historical comparability.
Data sources
In 2020–21, the ABS pooled a standard set of information from a number of existing surveys to produce the Smoker Status, Australia 2020–21 data set.
Surveys included in this pooled data set are:
- National Health Survey (NHS)
- General Social Survey (GSS)
- Survey of Income and Housing (SIH)
- Time Use Survey (TUS)
- National Study of Mental Health and Wellbeing (NSMHW).
Data items included as part of the Smoker Status, Australia 2020–21 pooled data set include:
- Demographics, such as Age, Sex, Country of Birth, Main language spoken and Marital status
- Household details, such as Type, Size, Household composition, Tenure, socio-economic indexes for areas (SEIFA), Geography
- Labour force status
- Educational attainment
- Self-assessed health status
- Migrant and Visa status
- Current smoker status.
The total sample pooled from the five surveys was 30,564 households and 42,117 persons (ABS 2021b).
Estimation methods
As only a sample of people in Australia were surveyed, their results needed to be converted into estimates for the whole population. This was done through a process called weighting:
- each person or household was given a number (known as a weight) to reflect how many people or households they represent in the whole population.
- a person or households’ initial weight was based on their probability of being selected in the sample. For example, if the probability of being selected in the survey was one in 45, then the person would have an initial weight of 45 (that is, they would represent 45 people).
The person and household level weights were then calibrated to align with independent estimates of the in-scope population, referred to as ‘benchmarks’. The benchmarks used additional information about the population to ensure that:
- people or households in the sample represented people or households that were similar to them
- the survey estimates reflected the distribution of the whole population, not the sample.
Benchmarks align to the estimated resident population (ERP) at December 2020, aged 15 years and over, which was 9,782,954 households and 20,285,817 people (after exclusion of people living in non-private dwellings, very remote areas of Australia and discrete Aboriginal and Torres Strait Islander communities).
There was no imputation for missing data on the pooled data set. Any records with an unacceptable level of missing data were removed. However, if the level of missing data was minimal, the records were kept with ‘not stated’ values where needed (ABS 2021b).
The smoking proportions for the Smoker Status, Australia 2020–21 and the 2020–21 National Health Survey data sets were aligned through the weighting process and benchmarks applied, in that the 2020–21 NHS smoking data was benchmarked in such a way as to match the current daily smoker data from the pooled data set. However, with perturbation for confidentiality reasons, the smoking proportions produced from the separate data sets will not match exactly.
Historical comparability
To maintain the safety of survey respondents and ABS Interviewers due to COVID-19, surveys that form part of the pooled Smoker Status, Australia 2020–21 data set were primarily collected via online, self-complete forms with some telephone and face-to-face interviews conducted where possible. Non-response is usually reduced through Interviewer follow up of households who have not responded. As this was not possible during COVID lockdown periods, there were significant impacts on response rates and sample representativeness. The Smoker Status, Australia 2020–21 data set has also expanded data sources, collection methodologies and content when compared with previous iterations of ABS Smoking data. As such, it should not be used to create a time series with previous data for smoking trends. The Smoker Status, Australia 2020–21 data set is considered a break in series, and reflects the specific time point only (ABS 2021b).
For more information, see Microdata: Smoker Status on the ABS website.
Things to consider when interpreting this data
- Data may be collected for a different purpose, not specifically for veterans’ smoking status.
- As the Smoker Status, Australia 2020–21 data set collects self-reported data, it is not possible to know how participants interpreted what constitutes ADF service, such as whether it is limited to overseas deployments or excludes reserve service. It is also not possible to distinguish between current serving and ex-serving personnel (AIHW 2018). This data set does not capture information about ADF members service characteristics such as rank, length of service, the number, length, and frequency of operational deployments nor income at time of separation. Each of these factors may be important to understanding rates of smoking among veterans.
- Data from the Smoker Status, Australia 2020–21 data set is based on self-reported veteran status, and all numbers are estimates that have been weighted to the Australian population. The sample selection, together with its weighting, is not intended to represent the veteran population, and therefore may over- or under-represent certain types of veterans.
- Veterans made up a small portion of the overall Smoker Status, Australia 2020–21 data set sample, which may cause some issues with the reliability and validity of results in this report. Any differences observed between this group and others mentioned in this report should be interpreted with caution and may be due to chance.
- Due to small counts of female veterans, sex disaggregation was unable to be done for most analysis in this report.
- It is possible that a difference between two sample-based results is due to chance rather than being a true difference. The ABS survey data presented in this report have been tested for significance at the 5% level using confidence intervals for the difference between two proportions. If the confidence interval of the difference between two proportions contains zero, the difference is statistically significant, but if the confidence interval does not contain zero, it is likely that the difference is not statistically significant (AIHW 2018). Statistically significant differences throughout this report have been indicated through the use of language such as ‘lower’ and ‘higher’ where comparisons between groups have been made.
- Data based on a sample rather than the whole population are subject to a degree of error, termed sampling error. This error describes the difference between the result obtained from the sample and the ‘true’ result for the whole population. The level of uncertainty associated with sampling error can be represented using Margin of Error (MoE) at the 95% confidence level. MoE is the distance from the population value that the sample estimate is likely to be within, specified at a given level of confidence (ABS 2021b). The 95% confidence interval is the estimate +/- MoE. In this report, confidence intervals display the range in which there is a 95% chance the true value lies.
- Proportions marked with a hash (#) have a high MoE and should be interpreted with caution. A high MoE is considered as greater than 10%.
- The findings in this report may differ from previously published figures due to previous age-standardisation results being used and different population groups being analysed. Different definitions may have also been used in some instances, and so results should not be compared to other publications.
- In this report, current daily smokers and current non-daily smokers have been aggregated to resolve small counts. However, current non-daily smokers are a small cohort, representing approximately 1% of current smokers who have ever served who are the focus in this report (ABS 2021b).
- Conclusions about the prevalence of smoking among veterans using the Smoker Status, Australia 2020–21 data set are limited, as the data set excludes e-cigarettes. E-cigarette use is also commonly referred to as vaping (DHAC 2021). Liquids used in e-cigarettes may contain nicotine and other toxic chemicals, and there is concern that the regular use of e-cigarettes could lead to adverse health consequences (CSIRO 2021).
| ABS | Australian Bureau of Statistics |
|---|---|
| ADF | Australian Defence Force |
| AIHW | Australian Institute of Health and Welfare |
| ARIA+ | Accessibility and Remoteness Index of Australia |
| DVA | Department of Veterans’ Affairs |
| IRSD | Index of Relative Socio-Economic Disadvantage |
| NDSHS | National Drug Strategy Household Survey |
| NHS | National Health Survey |
| SEIFA | Socio-Economic Indexes for Areas |
Glossary
Please refer to Glossary
| .. | not applicable |
|---|---|
| * | A statistically significant difference between men who have served in the ADF and have never served in the ADF, calculated using the confidence interval of the difference between the two proportions |
| # | Proportion has a high margin of error and should be used with caution |
| n.p. | not available for publication but included in totals where applicable, unless otherwise indicated |
ABS (Australian Bureau of Statistics) (2018). National Health Survey: First results, 2017–18 financial year, ABS, Australian Government, accessed 2 June 2022.
ABS (2021a) Microdata: Smoker Status, Australia, 2020–21, AIHW analysis of detailed microdata, accessed 2 May 2022.
ABS (2021b) Pandemic insights into Australian smokers, 2020–21, ABS, Australian Government, accessed 20 May 2022.
AIHW (Australian Institute of Health and Welfare) (2018) A profile of Australia's veterans 2018, AIHW, Australian Government, accessed 23 May 2022.
CSIRO (Commonwealth Scientific and Industrial Research Organisation) (2021) E-cigarettes, smoking and health, CSIRO website, accessed 11 July 2022.
DHAC (Department of Health and Aged Care) (2021) About e-cigarettes, DHAC, Australian government, accessed 11 July 2022.
Quit (2022), Coronavirus (COVID-19) and smoking – information for health professionals, Quit website, accessed 31 May 2022.
Vaneckova P, Sarich P, Cabasag C J, Liebermann E, Carle C, Hughes S, Egger S, O'Connell D, Weber M, da Costa A M, and Caruana M (2021), A systematic review and meta-analysis of tobacco smoking behaviour changes during the COVID-19 pandemic, International Journal of Epidemiology, 50(1), doi: 10.1093/ije/dyab168.679.
Yang H and Ma J (2021) ‘How the COVID-19 pandemic impacts tobacco addiction: Changes in smoking behavior and associations with well-being’, Addictive Behaviors, 119, 106917, doi: 10.1016/j.addbeh.2021.106917.