Summary
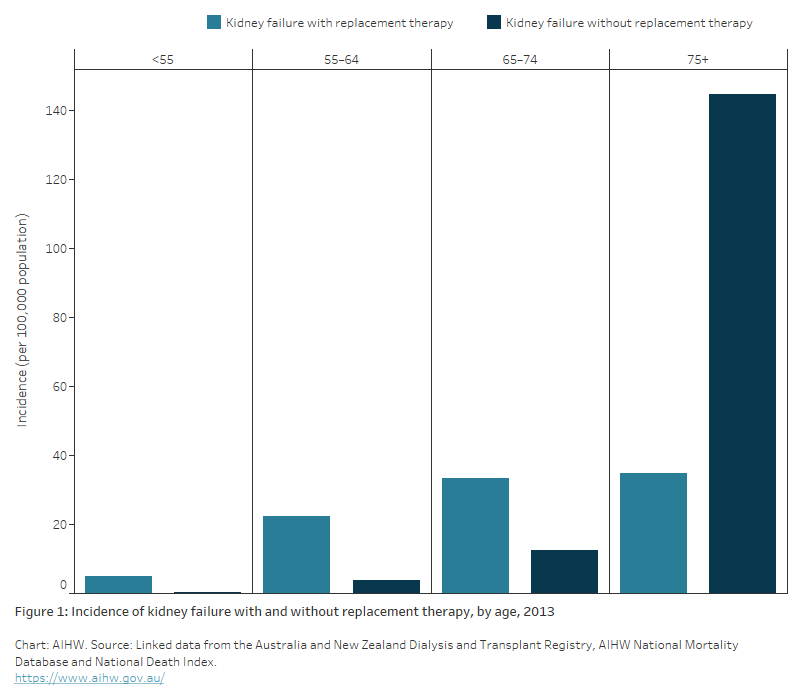
The bar chart shows the incidence rate of kidney failure in 2013 by sex, age group and kidney replacement therapy (KRT) treatment status, from the AIHW analysis of the linked ANZDATA, AIHW National Mortality Database and National Death Index.
The treatment rate for new patients with kidney failure increased slightly with age from 4.8 per 100,000 population among persons aged under 55, to 35 per 100,000 population among persons aged 75 and over. In contrast, the rate of new patients with kidney failure who did not get any KRT treatment increased sharply from 0.4 per 100,000 population among those aged under 55 to 145 per 100,000 population among those aged 75 and over. These age patterns are similar for men and women, with higher kidney failure incidence rates observed for males.
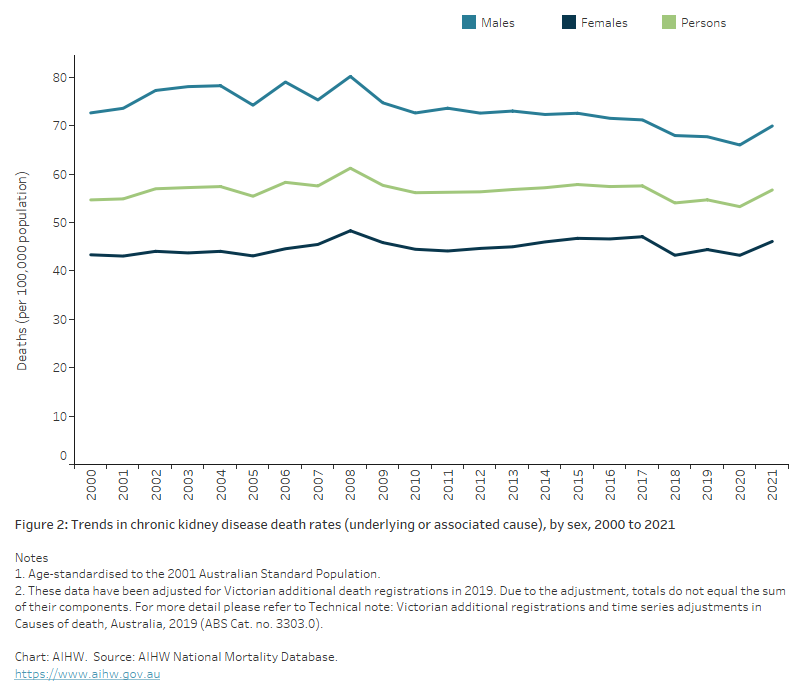
This graph shows the age-standardised rate of deaths where CKD was recorded as either an underlying or associated cause of death, from 2000 to 2021. Rates are higher in males than in females and have remained relatively stable. For persons, the rate of CKD deaths per 100,000 population was 55 in 2000, and 57 in 2021. The highest rate was in 2008, with 61 deaths per 100,000 population.
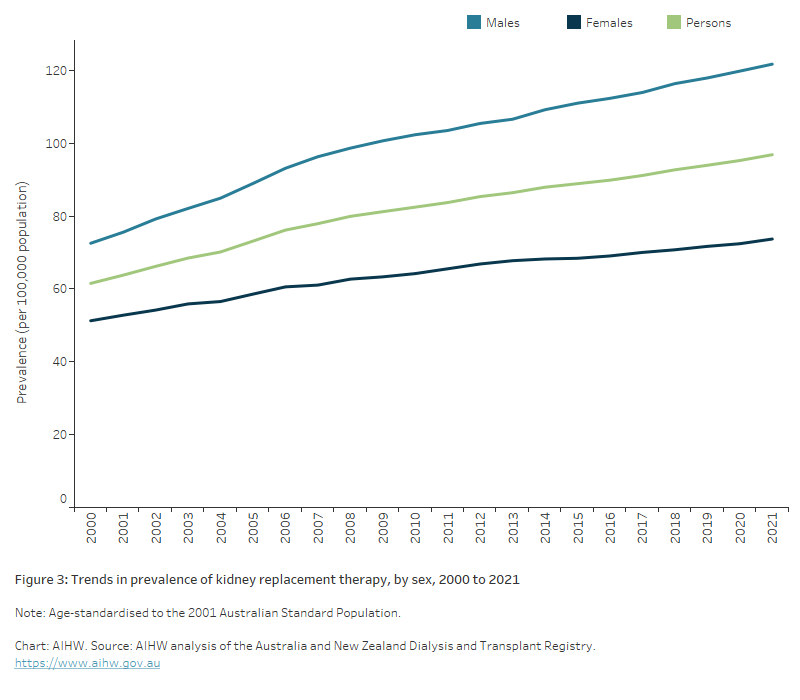
This graph shows the increasing trend of persons with kidney failure who are receiving kidney replacement therapy (KRT), by sex, from 2000 to 2021. The age-standardised rates have increased by 57%, from 62 per 100,000 in 2000 to 97 per 100,000 in 2021, with rates consistently higher in males than females. In 2021, the rate of persons with kidney failure receiving KRT was approximately 1.7 times higher among males (122 per 100,000 population) than females (74 per 100,00 population).
This table shows the relative impact of CKD in selected population groups, in terms of rates of: 1) prevalence, 2) hospitalisation, 3) death, 4) kidney failure patients receiving kidney replacement therapy, and 5) burden of disease. For each impact, rates are shown as a ratio comparing First Nations people and non-Indigenous Australians, people living in Remote and Very remote areas compared to Major cities, and people living in the lowest compared to the highest socioeconomic areas. Across all measures, the impact of CKD was higher for First Nations people compared to non-Indigenous Australians, higher for people living in Remote and Very remote areas compared to Major cities, and higher for people living in the lowest socioeconomic areas compared to the highest.
