Summary
Oral health is an important component of overall health and quality of life. Poor oral health can affect adults and children alike, causing pain, embarrassment, and even social marginalisation. For children, the effects can be long term, and carry through to adulthood.
Aboriginal and Torres Strait Islander children are more likely than non-Indigenous children to experience tooth decay. Several factors contribute towards the poorer oral health of Indigenous children, including social disadvantage and lack of access to appropriate diet and dental services.
For the past 10 years, the Australian Government has helped fund oral health services for Indigenous children aged under 16 in the Northern Territory. The Northern Territory Remote Aboriginal Investment Oral Health Program (NTRAI OHP) complements the Northern Territory Government Child Oral Health Program, by providing preventive (application of full-mouth fluoride varnish and fissure sealants) and clinical (tooth extractions, diagnostics, restorations and examinations) services.
This report presents data from the NTRAI OHP from July 2012 to December 2018, and includes long-term analyses for 2009–2018.
How many Indigenous children received services?
In 2018, almost 12,000 services were delivered to Indigenous children in the Northern Territory under the NTRAI OHP. Of those:
- almost 5,700 children received around 6,400 full-mouth fluoride varnish services, a rise of about 700 children from 2017
- 1,545 children received more than 1,600 fissure sealant services, a fall of nearly 100 children from 2017
- almost 3,200 children received clinical services on almost 3,900 occasions of service—such as dental assessments, fillings, extractions, or preventive services—a fall of more than 100 children from 2017.

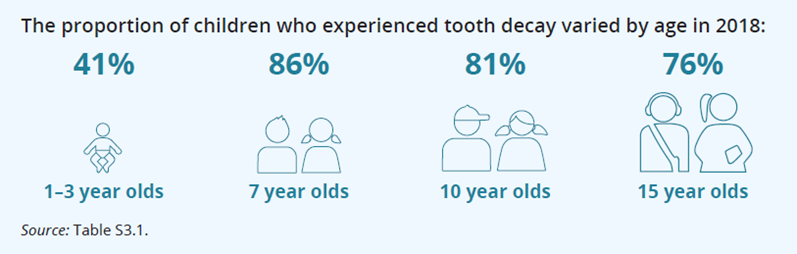
How many Indigenous children experienced tooth decay?
Tooth decay varied by age, and in 2018, children aged 7 and 8 had the highest percentage of tooth decay experience (86%). In comparison, 4 in 10 (41%) children aged 1–3 had tooth decay experience.
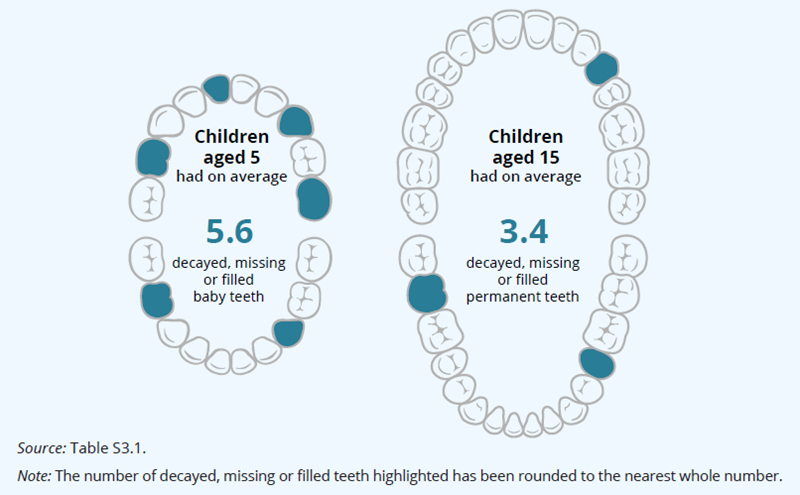
How many decayed, missing or filled teeth did Indigenous children have?
A widely used indicator to measure oral health status is a count of the number of decayed, missing or filled teeth.
On average, in 2018, children in the NTRAI OHP aged 5 had the highest average number of decayed, missing or filled baby teeth (dmft), at 5.6 teeth, while children aged 15 had the highest average number of decayed, missing or filled permanent teeth (DMFT), at 3.4.
Is the program meeting its benchmarks?
The NTRAI OHP has performance indicators and benchmarks to monitor its outcomes. In 2018, all of the clinical and preventive service delivery targets were met or exceeded (Table S1).
| Service delivery targets | Outcomes |
|---|---|
| At least 3,800 occasions of clinical service per year | 3,886 occasions of clinical services |
| At least 6,369 fluoride varnish applications in 2018 | 6,429 fluoride varnish applications provided |
| Fissure sealant applications to at least 4,000 teeth in 2018 | Fissure sealant applications to 6,927 teeth |
| Health outcome targets | |
| At least 50% of total service items are preventive services | 69% of total service items were preventive in 2018 |