Australia's mothers and babies:
Stillbirths and neonatal deaths
Web article
Last updated:
Topic: Mothers & babies
Part of Australia's mothers and babies
Citation
AIHW
Australian Institute of Health and Welfare (2023) Stillbirths and neonatal deaths, AIHW, Australian Government, accessed 27 April 2024.
APA
Australian Institute of Health and Welfare. (2023). Stillbirths and neonatal deaths. Retrieved from https://pp.aihw.gov.au/reports/mothers-babies/stillbirths-and-neonatal-deaths
MLA
Stillbirths and neonatal deaths. Australian Institute of Health and Welfare, 23 November 2023, https://pp.aihw.gov.au/reports/mothers-babies/stillbirths-and-neonatal-deaths
Vancouver
Australian Institute of Health and Welfare. Stillbirths and neonatal deaths [Internet]. Canberra: Australian Institute of Health and Welfare, 2023 [cited 2024 Apr. 27]. Available from: https://pp.aihw.gov.au/reports/mothers-babies/stillbirths-and-neonatal-deaths
Harvard
Australian Institute of Health and Welfare (AIHW) 2023, Stillbirths and neonatal deaths, viewed 27 April 2024, https://pp.aihw.gov.au/reports/mothers-babies/stillbirths-and-neonatal-deaths
Content warning: This content contains information some readers may find distressing as it relates to stillbirth and the loss of a baby.
In 2021, in Australia, 3,016 babies died in the perinatal period. Three-quarters (2,278) were stillbirths and the remaining 738 were neonatal deaths. This article provides information related to these deaths, including causes, maternal characteristics, timing and investigations.
The data presented in this article are from the National Perinatal Mortality Data Collection. It follows publication of preliminary data on perinatal deaths from the National Perinatal Data Collection, available in the Preliminary perinatal deaths section of this web report.
Overview of perinatal deaths
Australia is one of the safest places in the world for a baby to be born, yet death occurring within the perinatal period (from 20 weeks of gestation to 28 days after birth) is not uncommon. On an average day in Australia, 6 babies are stillborn and 2 die within 28 days of birth (neonatal death).
In 2021, there were:
- 315,705 babies born to 311,360 women
- 3,016 perinatal deaths (1% of babies born). Of these deaths, just over three-quarters (76%) were stillbirths (2,278) and 24% (738) were neonatal deaths (Figure 1)
- 9.6 perinatal deaths per 1,000 births (7.2 stillbirths per 1,000 births and 2.4 neonatal deaths per 1,000 live births).
Figure 1: Overview of perinatal deaths in 2021
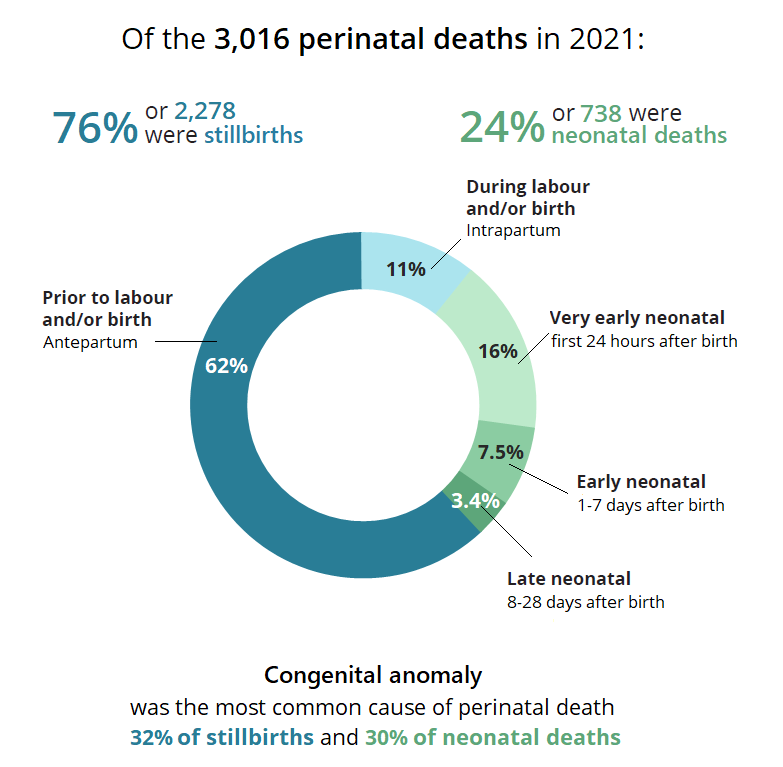
Note: Proportions for the timing of perinatal deaths (shown in the donut chart) do not add to the totals shown at the top of the figure, as they were calculated after excluding perinatal deaths where timing is not stated or unknown.
Chart: AIHW. Source: AIHW analysis of the National Perinatal Mortality Data Collection.
How have perinatal mortality rates changed over time?
Trends in this report cover a 20-year period from 2002 to 2021. However, data for 2002 are missing from some states and territories and hence 2003 is used as a baseline for comparison.
Between 2003 and 2021 the rate of perinatal death has varied between 9.1 and 10.5 deaths per 1,000 births, with a slight decrease from 2003 (Figure 2). The rate has decreased over this period for two categories in particular:
- stillbirths occurring at 28 weeks’ gestation or more
- neonatal deaths of babies born at 23 weeks’ gestation or more.
The overall stillbirth rate has remained between 6.7 and 7.7 per 1,000 births between 2003 and 2021. The rate in 2021 (7.2 per 1,000 births) is lower than in 2020 (7.7) – which marked a 20-year high-point – and the same as in 2019. The high rate in 2020 coincided with events such as the severe bushfires and the first year of the COVID-19 pandemic in Australia. These changes are similar to year-to-year fluctuations observed in the stillbirth rate since 2003. The rate of stillbirths occurring from 28 weeks’ gestation (third trimester) has continued to decline.
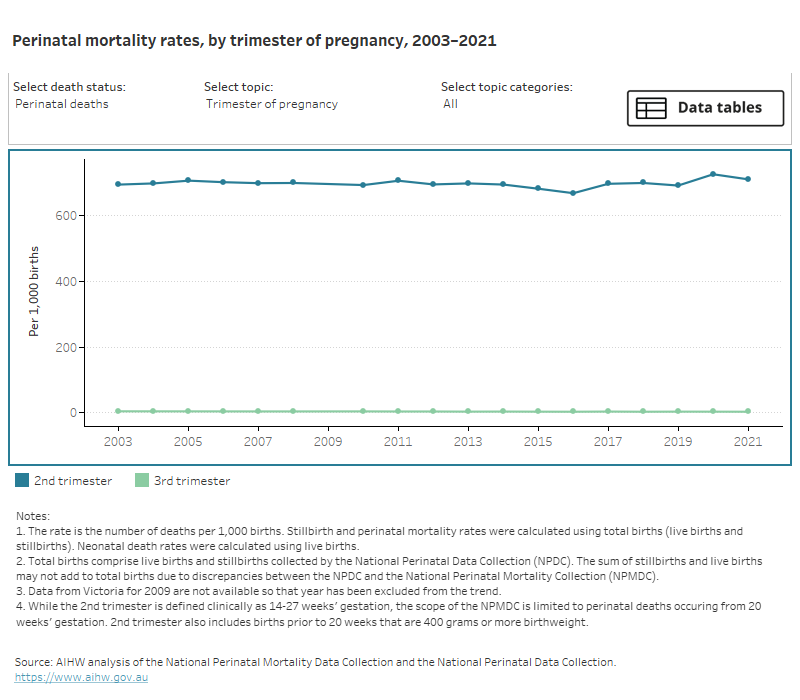
Figure 2: Perinatal mortality rates in Australia 2003–2021
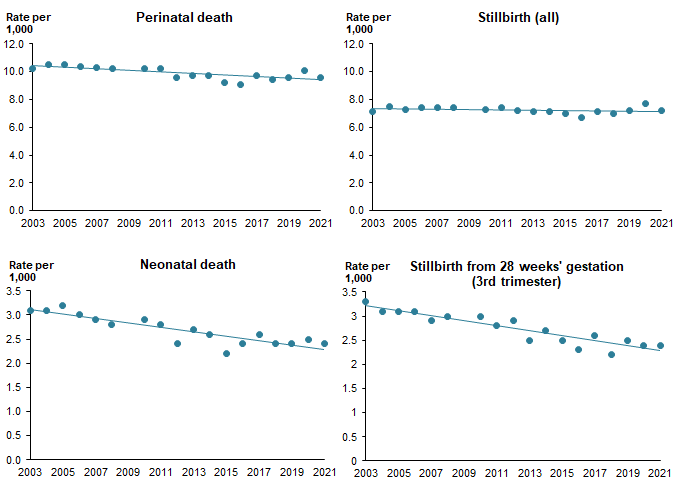
Notes:
- The rate is the number of deaths per 1,000 births. Stillbirth and perinatal death rates were calculated using total births (live births and stillbirths). Neonatal death rates were calculated using live births.
- Data for 2002 and 2009 were excluded from the model as data are missing from some states and territories for these years.
- The stillbirth rate reported for stillbirths from 28 weeks’ gestation is similar to the rate reported using the WHO definition for international comparison. For more information see Perinatal mortality rates for international comparison.
Chart: AIHW. Source: AIHW analysis of the National Perinatal Mortality Data Collection and the National Perinatal Data Collection
For data on perinatal mortality rates over time see tables 1 and 5 of the supplementary data tables (Data tables: National Perinatal Mortality Data Collection annual update 2021).
Perinatal mortality rates for international comparison
Definitions of perinatal mortality
Perinatal mortality rates in Australia are reported here using 2 distinct definitions for stillbirth.
The first (termed the Australian definition) defines stillbirth as a fetal death prior to birth of a baby born at 20 weeks’ gestation or more, and/or weighing 400 grams or more. This is the standard definition used for stillbirths in Australia.
A second definition for stillbirth is that used by the World Health Organisation (WHO), where stillbirths are defined as those occurring in the third trimester – born at 28 weeks’ gestation or more, and/or weighing 1,000 grams or more (WHO 2018). This definition is used for the purposes of international reporting and comparison.
Reporting of neonatal deaths is the same for both the Australian and WHO definitions. Neonatal deaths are all registered deaths occurring within 28 days of birth (WHO 2018). In Australia, registered deaths are those born at 20 weeks’ gestation or more, and/or weighing 400 grams or more.
Using the WHO definition of stillbirth excludes the smaller and less mature babies who are included when the standard definition applied in Australia is used. Australian perinatal mortality rates reported using the WHO definitions are therefore lower than those reported using the Australian definitions.
Refer to the Technical notes – Definitions for more information on WHO definitions of perinatal mortality.
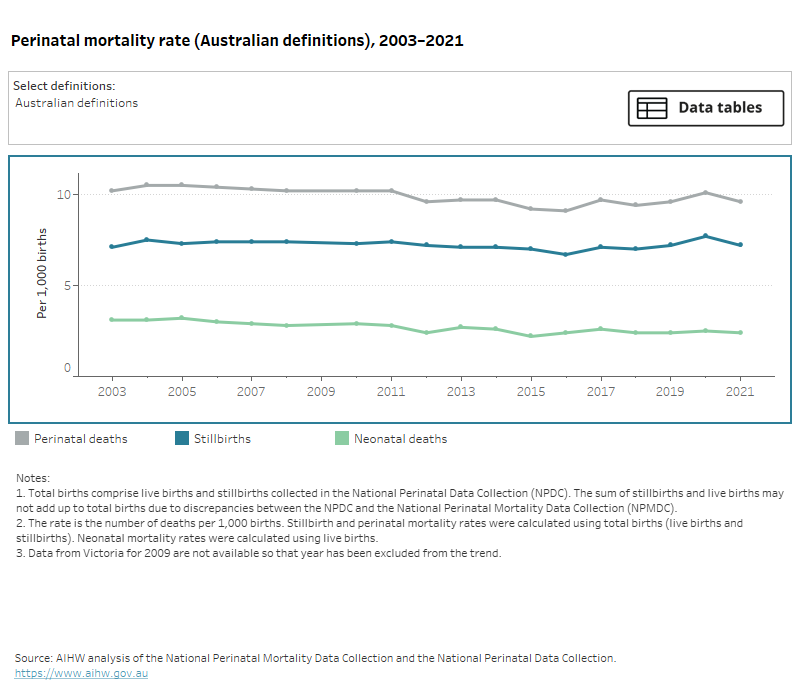
The rate of stillbirths in Australia, using the WHO definition (stillbirth born at 28 weeks’ gestation or more, or 1,000 grams birthweight or more), has decreased from 3.3 per 1,000 births in 2003 to 2.5 per 1,000 births in 2021.
By comparison, using the Australian definition the rate of stillbirths has not followed a single trend over this period, ranging between 6.7 and 7.7 per 1,000 births.
The rate of neonatal deaths in Australia decreased from 3.1 per 1,000 live births in 2003 to 2.4 per 1,000 live births in 2021. The rate of neonatal deaths in Australia is the same using both the Australian and WHO definitions.
Data on perinatal mortality rates over time using the Australian and WHO definitions can be explored in the interactive data visualisation below (Figure 3), with data also presented in tables 1 and 2 of the supplementary data tables (Data tables: National Perinatal Mortality Data Collection annual update 2021).
Figure 3: Perinatal mortality rates in Australia, by selected definition, 2003–2021
Rates of stillbirth, neonatal death, and overall perinatal death between 2003 and 2021, using either the Australian or WHO definitions.
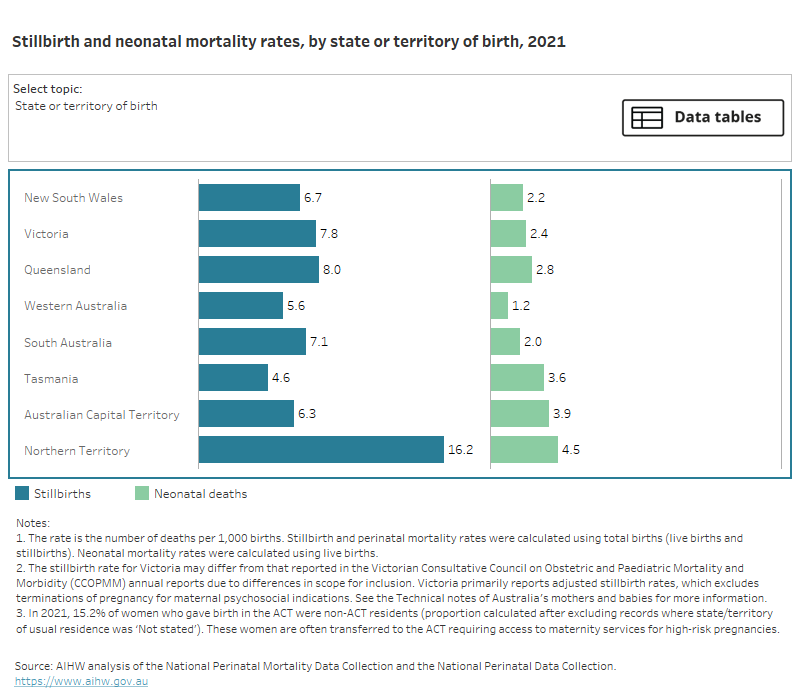
Rates of stillbirth and neonatal death in 2021 by various maternal demographic characteristics, including state/territory of birth.
Rates of stillbirth and neonatal death in 2021 by characteristics of the baby and pregnancy, including birthweight, gestation, and plurality.
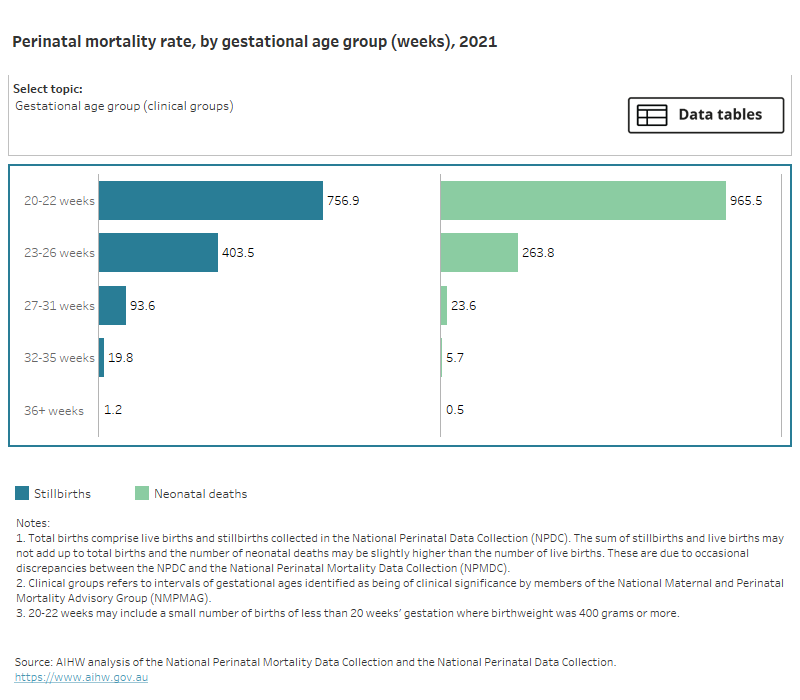
Rates of stillbirth, neonatal death, or overall perinatal death between 2003 and 2021, by gestational age.
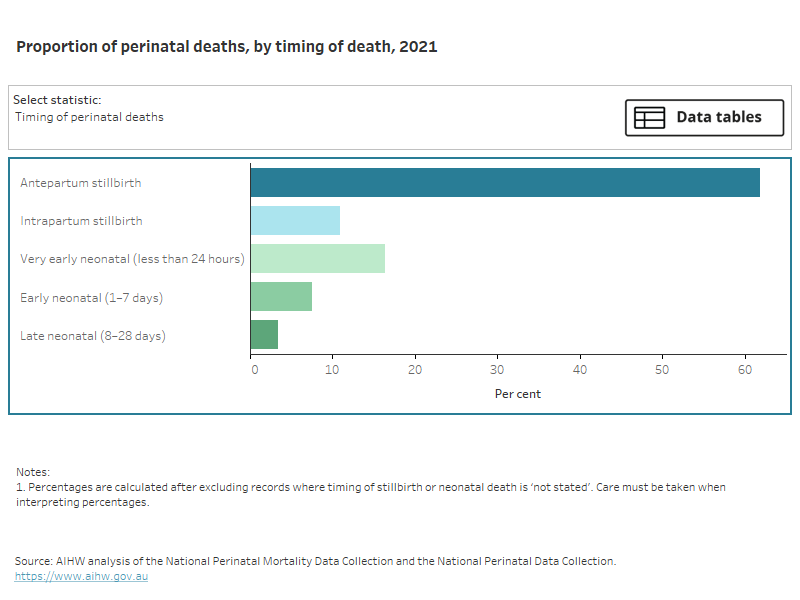
Timing of perinatal death as a proportion of all perinatal deaths in 2021. In a separate view, these data are broken down by gestational age group.
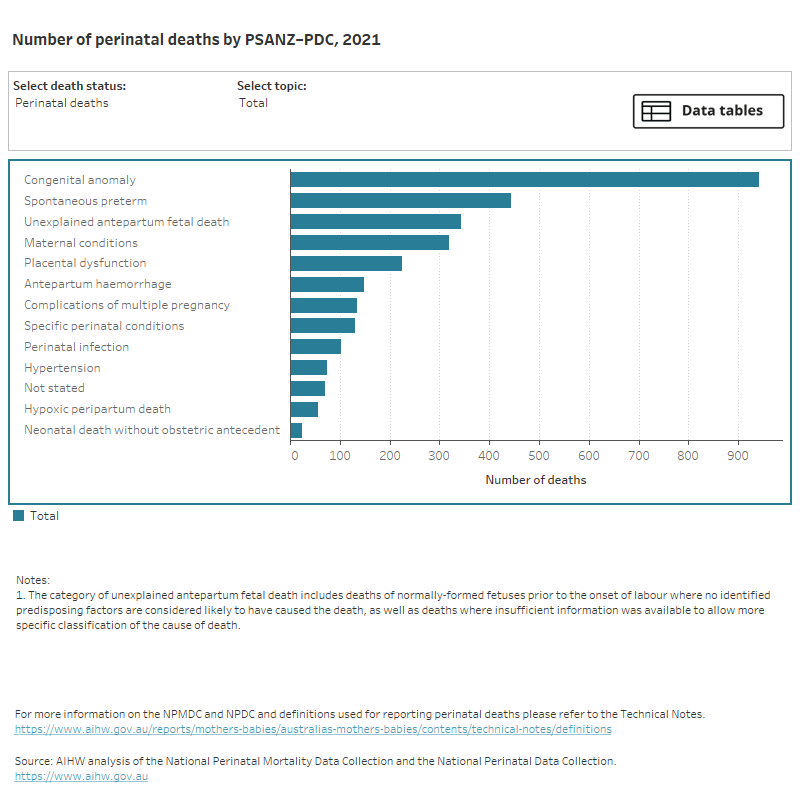
Causes of perinatal deaths in 2021. In separate views, these data are broken down by various characteristics including gestation, birthweight percentile.
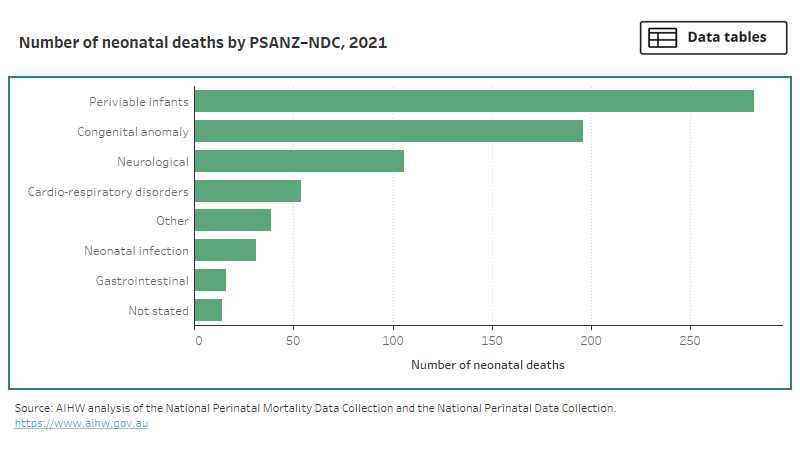
Causes of neonatal deaths in 2021. Periviable infants (typically <24 weeks’ gestation) was the most commonly classified condition.
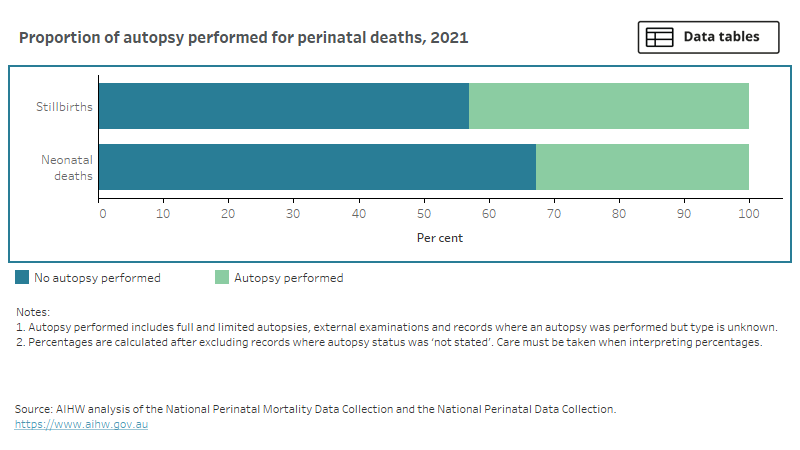
Proportions of stillbirths and neonatal deaths in 2021 for which an autopsy was performed. In the majority of cases autopsies were not performed.