Health of people experiencing homelessness
Web article
Release Date:
Section: Health status
Citation
AIHW
Australian Institute of Health and Welfare (2024) Health of people experiencing homelessness, AIHW, Australian Government, accessed 27 April 2024.
APA
Australian Institute of Health and Welfare. (2024). Health of people experiencing homelessness. Retrieved from https://pp.aihw.gov.au/reports/australias-health/health-of-people-experiencing-homelessness
MLA
Health of people experiencing homelessness. Australian Institute of Health and Welfare, 27 February 2024, https://pp.aihw.gov.au/reports/australias-health/health-of-people-experiencing-homelessness
Vancouver
Australian Institute of Health and Welfare. Health of people experiencing homelessness [Internet]. Canberra: Australian Institute of Health and Welfare, 2024 [cited 2024 Apr. 27]. Available from: https://pp.aihw.gov.au/reports/australias-health/health-of-people-experiencing-homelessness
Harvard
Australian Institute of Health and Welfare (AIHW) 2024, Health of people experiencing homelessness, viewed 27 April 2024, https://pp.aihw.gov.au/reports/australias-health/health-of-people-experiencing-homelessness

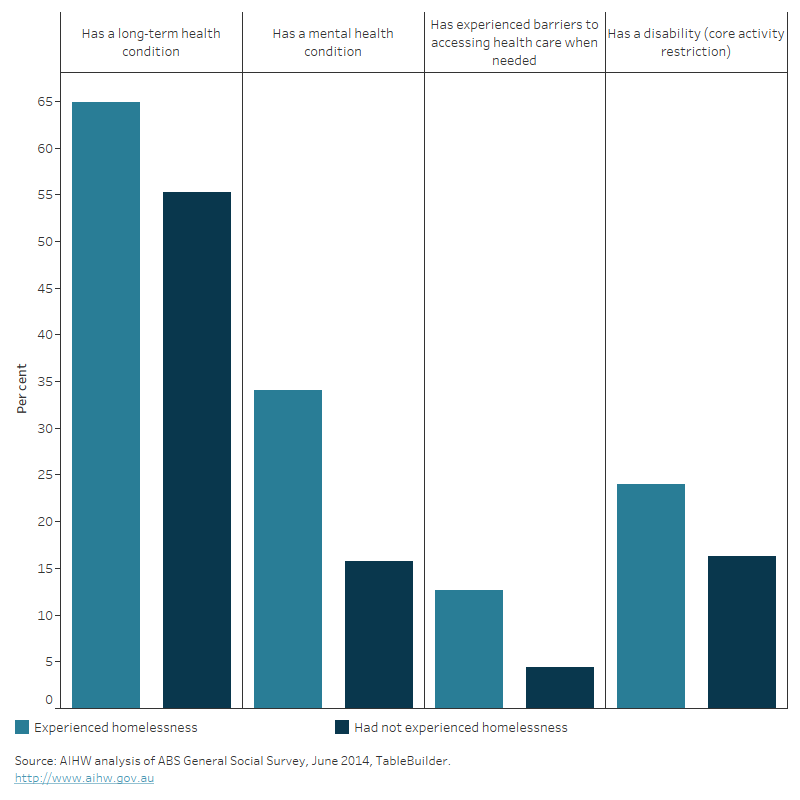
The bar chart shows there was a higher proportion of individuals self- reporting a long-term health condition, a mental health condition, disability or having experienced barriers when accessing health care when needed amongst those who had experienced homelessness compared with those who had not experienced homelessness.
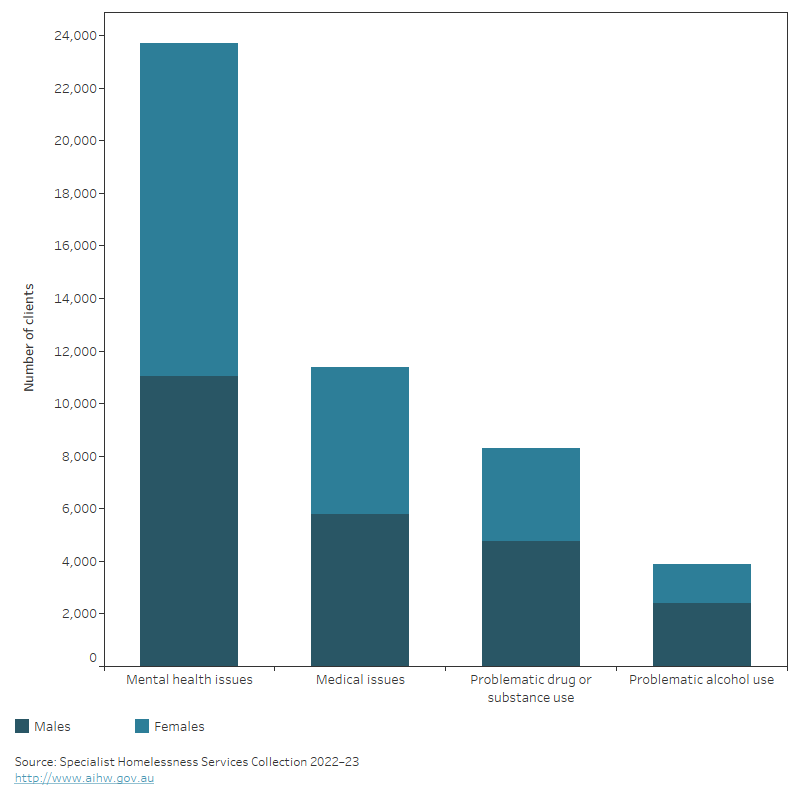
The stacked vertical bar graph shows the number of male and female clients who were homeless at first presentation to a specialist homelessness service by health-related reasons for seeking assistance. For both males and females, the most common health-related reason for seeking assistance was mental health issues, followed by medical issues, problematic drug or substance use and problematic alcohol use. These reasons for seeking assistance were more commonly reported for males than females except for mental health issues.