Overarching methods and choices for risk factors
A risk factor is any determinant that causes (or increases the likelihood of) one or more diseases or injuries. As well as providing estimates of fatal and non-fatal burden, burden of disease methodology allows death and health loss to be attributed to specific underlying (or linked) risk factors. Quantification of the impact of risk factors assists evidence-based decisions about where to direct efforts to prevent disease and injury and to improve population health.
The methods used to quantify the impact of risk factors in the ABDS 2018 are described in this chapter (see specific risk factor methods for detail on each risk factor).
Box 2.3: Key terms used in this chapter
attributable burden: The disease burden attributed to a particular risk factor. It is the reduction in burden that would have occurred if exposure to the risk factor had been avoided or had been reduced to its theoretical minimum risk exposure distribution (TMRED).
counterfactual: An alternative risk factor exposure distribution chosen for comparison with the observed distribution, to estimate the alterable contribution of that risk factor to the burden of disease. The most commonly used counterfactual in burden of disease studies is the theoretical minimum risk exposure distribution (TMRED).
effect modification: A change in the observed magnitude or direction of an association between a risk exposure and an outcome when a third variable (such as age or sex) is included in the analysis.
effect size: A statistical measure of the strength of the relationship between 2 variables (in this context, between a risk exposure and a disease outcome), expressed, for example, as a relative risk or odds ratio.
linked disease: A disease or injury for which there is evidence that its likelihood is increased by the risk factor in question.
population attributable fraction (PAF): For a particular risk factor and causally linked disease or injury, the percentage reduction in burden that would occur for a population if exposure to the risk factor was avoided or reduced to its theoretical minimum.
relative risk (RR): The risk of an event relative to exposure, calculated as the ratio of the probability of the event’s occurring in the exposed group to the probability of its occurring in the unexposed group.
risk exposure distribution: The measure of the spread or distribution of exposure to the risk factor in the population that have encountered or experienced, or have the risk factor.
risk factor: Any factor that causes or increases the likelihood of illness or death due to a disease or injury or other unwanted condition or event.
theoretical minimum risk exposure distribution (TMRED): The risk factor exposure distribution that will lead to the lowest conceivable disease burden
The burden attributable to risk factors is generally estimated using PAFs applied to the disease burden estimated as described in the disease burden sections.
Methodological developments in the ABDS 2018
Most of the risk factors methods were the same as those used in the ABDS 2015. However, some methods have changed following new risk factor methods by GBD 2019 and expert advice (GBD 2019 Risk Factors Collaborators 2020).
The most notable of these was the changes to physical inactivity and the dietary risk factors which both had changes to the categories of exposure that increased risk and the minimum exposure associated with increased risk (TMRED). These changes are described in detail in Risk factor specific methods section, a summary of the major changes are outlined below.
The methods for the dietary risk factor Diet high in sugar sweetened beverages changed to be directly linked to type 2 diabetes and coronary heart disease instead of mediating through overweight (including obesity).
Exposure to air pollution was also estimated from satellites calibrated with ground monitoring stations, instead of ground monitoring stations alone, improving the coverage of estimates for Australia.
Two new risk factors have been included: bullying victimisation and low birthweight & short gestation. Both risk factors were included in GBD 2019; however, the methods used in ABDS 2018 for bullying victimisation were based on Australian specific studies (Jadambaa 2019a, Jadambaa 2019b).
Steps in estimating risk factor attributable burden
The basic steps of estimating risk factor attributable burden are:
- select risk factors
- identify linked diseases based on convincing or probable evidence in the literature that the risk factor has a causal association with increased prevalence or mortality
- define the exposure to the risk factor that is not associated with increased risk of disease (the theoretical minimum risk exposure distribution, or TMRED, or counterfactual)
- estimate the PAFs by either a direct method or the comparative risk assessment method:
- if PAFs appropriate to the disease and population in question are available from a comprehensive data source (such as a disease register), they are estimated directly from this data source (named a direct PAF in this report) and do not require steps 5, 6 and 7
- if not, PAFs are created using the comparative risk assessment method, which involves steps 5, 6 and 7
- define the amount of increased risk (relative risk) of morbidity or mortality for the linked disease due to exposure to the risk factor
- estimate exposure to each risk factor in the population
- use these inputs to calculate the PAF. The PAF has a value between 0 and 1, where 0 means there was no burden attributable to the risk factor and 1 means that all the burden for the linked disease was attributable to the risk factor.
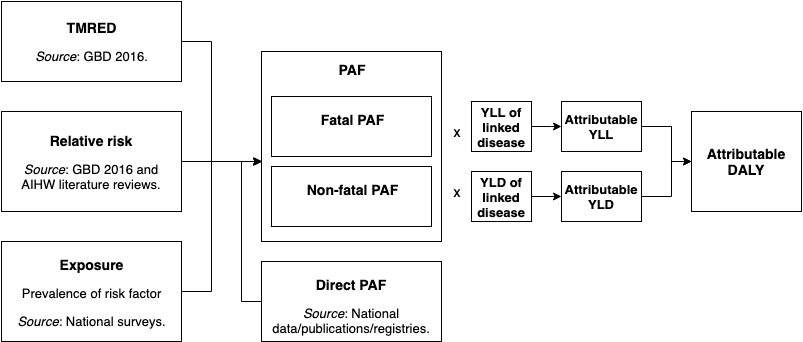
The burden attributable to each risk factor is calculated by applying the PAFs for each linked disease to the relevant YLL and YLD.
This process is shown in the figure below.
Figure 2.2: Inputs and processes to calculate attributable burden
Selection of risk factors
The risk factor list describes the specific risk factors considered as underlying causes of health loss through their causal association with particular diseases. In contrast to the disease list, which is exhaustive, and where an established classification system (the International Statistical Classification of Diseases and Related Health Problems) exists, the list of potential risk factors is near limitless, and there is often no consensus in the literature on what level(s) of exposure constitute ‘risk’. A predetermined set of criteria was used to develop the list, taking into account the potential for modification of exposure in the population, the availability of data on exposure, and the quality of evidence about the presence and magnitude of causal effects.
To be included in the ABDS 2018, a risk factor had to satisfy one or more of the following criteria:
Included in other studies’ risk factor lists
- Have been included in:
- the GBD 2019
- the ABDS 2011 or ABDS 2015 unless its inclusion in the ABDS 2018 conflicted with other criteria.
Substantial impact and policy interest
- Be of considerable importance to national or Indigenous disease burden based on previous studies (ABDS 2011, ABDS 2015; GBD 2019).
- Be of substantial Australian or Indigenous health policy interest – defined as currently being the focus of policy concern, professional attention or monitoring activity.
- Be modifiable, and able to be prevented or modified through policy intervention.
Be able to be measured
- Be measurable, including having:
- sufficient evidence for causal association between exposure and health outcomes based on high-quality epidemiological studies
- enough data and methods to enable exposure distributions to be estimated
- enough data to estimate effect sizes per unit of exposure of outcome-specific impacts
- evidence to support the ability of effect sizes to be generalised to populations, other than those included in the available studies, or to satisfactory models for extrapolating them.
ABDS 2018 risk factor list
The ABDS 2018 identified 40 risk factor components or exposures (such as cannabis and cocaine use) that combine to 20 individual risk factors (such as illicit drug use). These were broadly grouped into categories (behavioural, metabolic/biomedical and environmental risks).