Hospitalisations
Page highlights
- There were 40,500 endometriosis-related hospitalisations in 2021–22. This represents 312 hospitalisations per 100,000 females.
- 82% of endometriosis-related hospitalisations were amongst females aged 15–44, representing 18 out of every 1,000 hospitalisations in this age group.
- The number of endometriosis-related hospitalisations increased by 43% between 2011–12 and 2021–22, from 28,400 to 40,500 hospitalisations, peaking at 43,800 in 2020–21.
- The rate of endometriosis hospitalisations has doubled among females aged 20–24 in the past decade, from 330 hospitalisations per 100,000 females in 2011–12 to 660 per 100,000 in 2021–22.
- There were just over 1,000 endometriosis-related hospitalisations for First Nations people, representing 2.5% of endometriosis-related hospitalisations.
- In 2021–22, 26% of endometriosis-related hospitalisations were among females born outside of Australia.
- Over two-thirds (68%) of endometriosis-related hospitalisations took place in a private hospital.
Around half (52%) of endometriosis-related hospitalisations in 2021–22 had endometriosis as the principal diagnosis according to the AIHW National Hospital Morbidity Database (NHMD). The remainder had endometriosis as an additional diagnosis only (48%). See Co-occurring diagnoses for information on other diagnoses commonly recorded for endometriosis-related hospitalisations.
About 1 in 3 (33%) hospitalisations with a principal diagnosis of endometriosis also had one or more additional diagnoses of endometriosis.
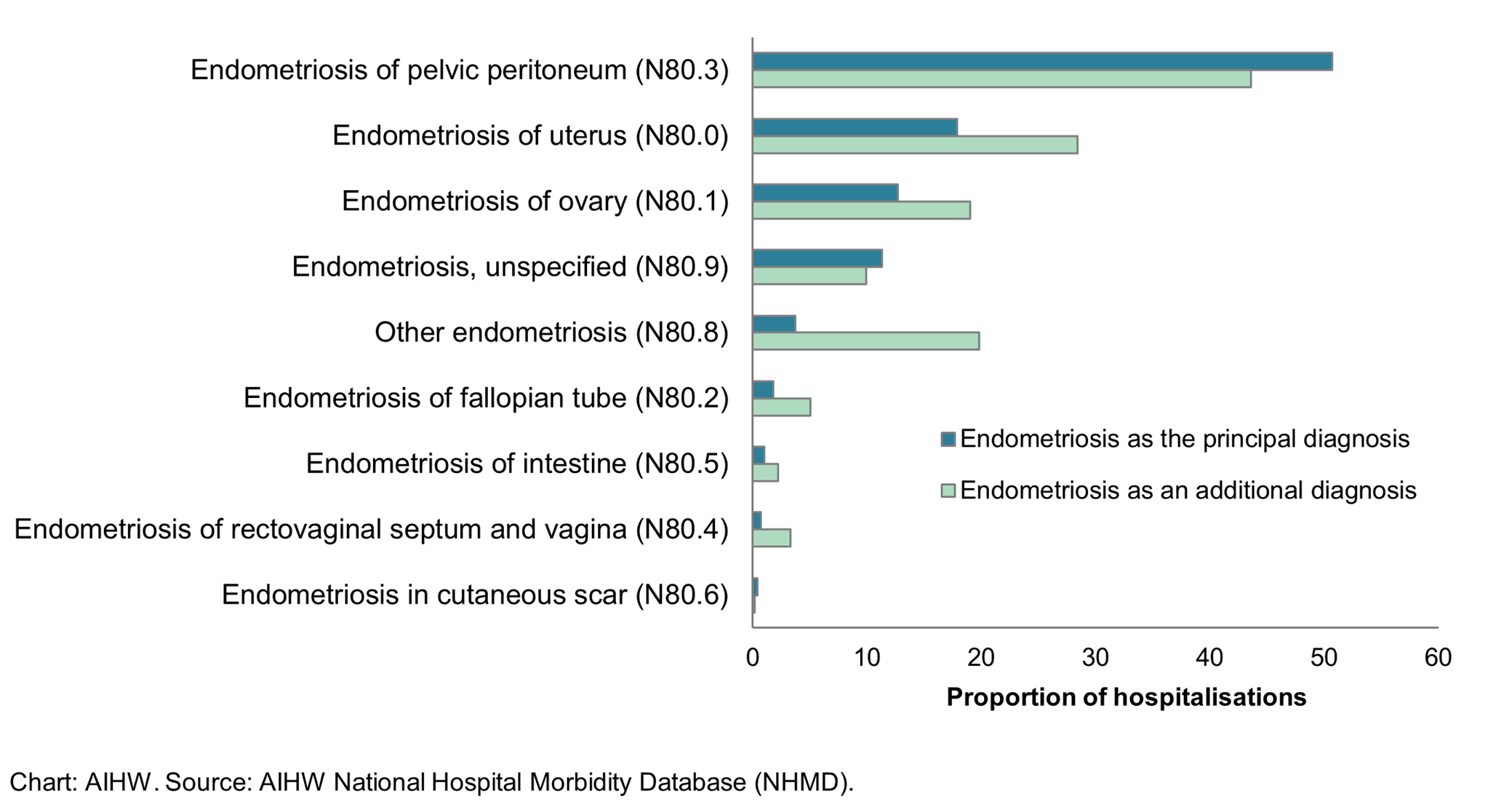
Endometriosis of the pelvic peritoneum was the most common diagnosis among the hospitalisations, representing 51% of principal diagnoses and 44% of additional diagnoses (Figure 2). This was followed by endometriosis of the uterus (18% of principal and 28% of additional diagnoses), and of the ovary (13% of principal and 19% of additional diagnoses).
Figure 2: Endometriosis-related hospitalisations, by 4th character ICD-10-AM code, 2021–22
Notes
- Endometriosis of uterus (N80.0) includes adenomyosis. Other endometriosis (N80.8) includes endometriosis of thorax.
- The total proportion for endometriosis as an additional diagnosis exceeds 100% as some hospitalisations have more than one additional diagnosis of endometriosis.
What is an endometriosis-related hospitalisation?
- Hospitalisation data presented here are based on admitted patient episodes of care from the National Hospital Morbidity Database (NHMD), including multiple events experienced by the same individual in a given time frame.
- A separation is an episode of care for an admitted patient, which can be a total hospital stay (from admission to discharge, transfer or death) or a portion of a hospital stay beginning or ending in a change of type of care (for example, from acute care to rehabilitation). In this report, separations are referred to as hospitalisations.
- Hospitalisations with endometriosis as the principal diagnosis are hospitalisations for which endometriosis was determined to be chiefly responsible for occasioning the episode of admitted patient care.
- Hospitalisations with endometriosis as an additional diagnosis only are hospitalisations for which another condition was chiefly responsible for the episode of care, but endometriosis was determined to affect patient management.
- Some hospitalisations have endometriosis listed as both a principal and additional diagnosis. These hospitalisations are counted with the principal diagnosis group and excluded from the additional diagnosis group to avoid double counting.
- Endometriosis-related hospitalisations are hospitalisations with a principal and/ or additional diagnosis of endometriosis.
- A procedure is a clinical intervention that is surgical in nature, carries a procedural risk, carries an anaesthetic risk, requires specialised training and/or requires special facilities or equipment only available in an acute care setting.
- The health classification used for morbidity reporting in Australia is the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM) which is used alongside the Australian Classification of Health Interventions (ACHI) which classifies procedures and interventions.
For further information on the NHMD and the methods used in this report, see the Technical notes.
Variation by age
Most endometriosis-related hospitalisations (82% in 2021–22) are among females aged 15–44 (Figure 3), which are generally regarded as a woman’s reproductive years. This represents 18 out of every 1,000 hospitalisations among females in this age group. In comparison, 31% of all hospitalisations among females in 2021–22 were for this age group. Endometriosis was the 20th most common reason for hospitalisation among those aged 15–44 years (by principal diagnosis at the ICD-10-AM 3-character level). The most common reasons for hospitalisation among this age group are related to childbirth, procreative management, dialysis, and abdominal and pelvic pain.
There are few endometriosis-related hospitalisations among females aged under 15. The number and the rate of hospitalisations then rise with age to 30–39, before decreasing. There are relatively few hospitalisations among women aged 55 and over, potentially reflecting the decrease in endometriosis symptoms among most women after menopause.
Over the past decade, the rate of endometriosis-related hospitalisations increased across most age groups. The greatest increase was seen among ages 20–24, with the rate doubling between 2011–12 and 2021–22 (from 330 to 660 hospitalisations per 100,000 females). In 2021–22, 21 out of every 1,000 hospitalisations among females aged 20–24 were related to endometriosis. This trend was particularly driven by the increase in the rate of hospitalisations in private hospitals for women aged 20–24, which more than doubled from 175 to 425 hospitalisations per 100,000 females in this period.
Total bed days mirrors the pattern seen for hospitalisations, with the peak generally among ages 35–39.
Figure 3: Age profile of endometriosis-related hospitalisations, 2011–12 to 2021–22
Alt text: This interactive line chart shows the number, crude rate, and total bed days of endometriosis hospitalisations by age group, hospital sector and year. In 2021–22 the overall number of hospitalisations, rate of hospitalisation and total bed days were highest among females aged 35–39.

This interactive line chart shows endometriosis-related hospitalisations by year and by hospital sector. The number and rate of hospitalisations for endometriosis were higher in private hospitals than public hospitals for all years. The median age was younger in public hospitals than private hospitals across all years. Similar patterns were seen for ages 15–44 as with all ages, and for a principal diagnosis of endometriosis as with any diagnosis of endometriosis.

Alt text: This interactive bar chart shows endometriosis-related hospitalisations by socio-economic group, remoteness area and Indigenous status. The crude rate of endometriosis hospitalisations was highest in the second most advantaged socioeconomic group and lowest in the most disadvantaged group. Crude hospitalisation rates were highest in Major cities and lowest in Remote and very remote areas. Similar patterns were seen for a principal diagnosis of endometriosis as with any diagnosis of endometriosis.

Alt text: This interactive bar chart shows endometriosis-related hospitalisations by region of birth in 2021–22. Measures included are number of hospitalisations, hospitalisations per 100,000 population (crude rate) and median age. Australia had the highest number of hospitalisations at 29,980. The Americas had the highest crude rate of hospitalisations at 395 per 100,000 population. Australia had the youngest median age out of all regions at age 33.
