Patient safety
This section presents data for the patient safety indicators supplied by Australia to the HCQO collection. It compares these data with the HCQO results for other OECD countries, and comments on the comparability of the data provided to the OECD specification (OECD 2021).
Patient safety remains a pressing issue in the delivery of health services, with over 15% of hospital expenditure and activity in OECD countries attributable to treating patients who experienced a safety event, many of which are preventable (OECD 2021). Patient safety indicators screen for events that patients experience during their hospital stays as a result of exposure to the health-care system – either adverse events that cannot be totally avoided or events that should never occur (OECD 2021).
The OECD published all patient safety indicators in OECD.Stat and a selection of these indicators in Health at a glance 2023. Australia submitted results for 6 of 8 patient safety indicators requested:
- Retained surgical item or unretrieved device fragment
- Post-operative pulmonary embolism – hip and knee replacement hospitalisations
- Post-operative deep vein thrombosis – hip and knee replacement hospitalisations
- Post-operative sepsis – abdominal hospitalisations
- Obstetric trauma after vaginal delivery with instrument
- Obstetric trauma after vaginal delivery without instrument.
The indicator definitions can be viewed here: Patient safety indicator definitions
Overall data comparability and methods
The most recent data supplied by Australia for the patient safety indicators were for 2020–21. These data are recorded as 2020 data in the OECD.Stat database, and so are described in that way here. Data from other OECD countries published on OECD.Stat for 2020 are used for comparison and calculation of OECD averages in this section. These data were extracted from the OECD.Stat database in January 2024, and may not reflect subsequent updates made to the database.
The OECD requested patient safety data for adults aged 15 and over, disaggregated by age and sex. These indicator rates were not age-sex standardised by the OECD. The indicators are presented on the same basis here.
It should be noted that data from the AIHW’s National Hospital Morbidity Database (NHMD) are collected primarily for the purposes of recording care provided to admitted patients, and that use of the data for HCQO purposes has not been validated for accuracy in Australia. The results should therefore be treated with caution. Health at a glance 2021 notes that ‘variations in definitions and medical recording practices between countries can affect calculation of rates and limit data comparability in some cases’ (OECD 2021:28). It further notes that ‘higher adverse event rates may signal more developed patient safety monitoring systems and a stronger patient safety culture rather than worse care’ (OECD 2021:28).
In Australia, there is a lack of financial disincentives connected to the reporting of adverse events, and this may have contributed to some relatively high rates reported for Australia. It is also possible that efforts to improve coding quality and to improve the focus on patient safety in Australia in recent years could have led to increased reporting of patient safety events in Australia compared with some other OECD countries.
A number of features of Australian patient safety monitoring would support the claim that Australia is one of those countries that has a more developed patient safety monitoring system. Australia employs specially trained staff to identify and code information from patient records. It is also likely that in Australia additional diagnoses are generally well recorded at the national level due to the ability to record up to 99 additional diagnoses for reporting to the NHMD.
The AIHW endeavoured to apply all specifications as supplied by the OECD; however, there were some parts where this was not able to be achieved. The OECD specifications for the patient safety indicators requested identification of readmissions in order to identify any subsequent related admissions to hospital within 30 days of the original hospital admission, as some adverse events are likely to manifest in the period following discharge from hospital. Australia’s national data collection for admitted patients (the NHMD) is based on a single episode of care as the statistical unit (as described in the Acute care section). Therefore, Australia was unable to meet this requirement, and could only include instances that occurred within the one (hospital) episode of care in the calculations of the patient safety indicators.
The OECD specifications also requested the exclusion of some cases where the condition of interest was present on admission; however, due to data quality issues, the AIHW did not do this, as not all cases that arose during the episode were flagged as such.
Retained surgical item or unretrieved device fragment
Sentinel events are a subset of adverse patient safety events that are wholly preventable and result in serious harm to, or death of, a patient (ACSQHC 2020). The ‘unintended retention of a foreign object in a patient after surgery or other invasive procedure resulting in severe harm or death’ is listed as one of the 10 sentinel events that are recommended for monitoring and reporting in Australia to drive national improvements in patient safety (ACSQHC 2020).
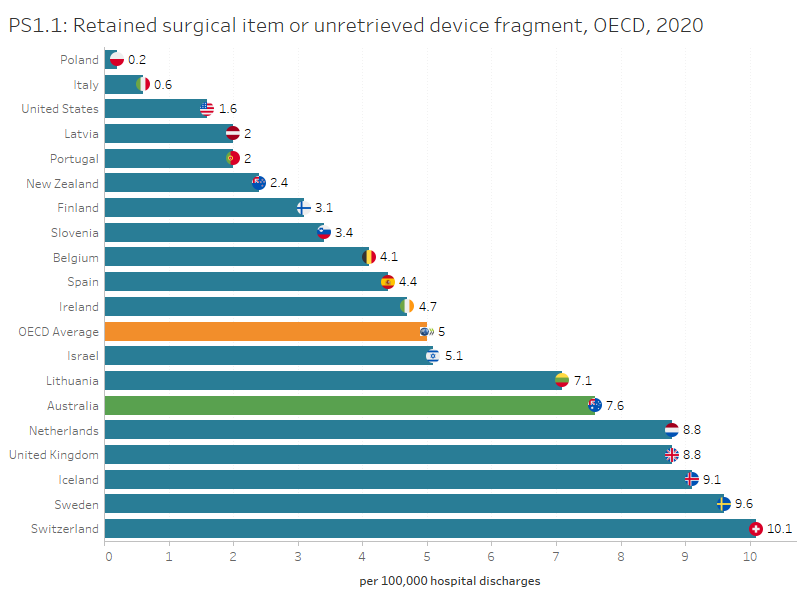
In Australia, the rate of retained surgical item or unretrieved device fragment for people aged 15 and over was 7.6 per 100,000 hospitalisations in 2020, higher than the OECD average of 5 per 100,000 hospitalisations. Australia had one of the highest rates of retained foreign objects among the OECD countries that submitted data for 2020 and Poland had the lowest rate with 0.2 per 100,000 hospitalisations.
In Australia, the rate has fluctuated over time in the past decade, ranging from 9.7 per 100,000 hospitalisations in 2013 to 7.4 per 100,000 hospitalisations in 2015.
Interactive PS1.1 below compares OECD countries that submitted data for this indicator for 2020, while PS1.2 presents Australia’s 10-year trend for this indicator.
Figures PS1.1 and PS1.2
PS1.1 presents OECD countries with data available for retained surgical item or unretrieved device fragment indicator in 2020, which shows Australia had the highest rate. PS1.2 presents Australia’s 10-year trend for this indicator, which shows a fluctuating trend over time.
Post-operative pulmonary embolism and deep vein thrombosis – hip and knee replacement hospitalisations
Pulmonary embolism (PE) is a blood clot that breaks off from the deep veins and travels round the circulatory system to block the arteries in the lung. Deep vein thrombosis (DVT) is a blockage in the deep veins of the legs, thighs, or pelvis, caused by the clotting of blood. Most deaths arising from DVT are caused by PE (NICE 2018).
The risk of PE and DVT following hip and knee replacement procedures is higher than following other surgical procedures (OECD 2013). Both conditions may result in pain, decreased mobility, and sometimes death, but both can be prevented by anticoagulants and other measures (OECD 2021).
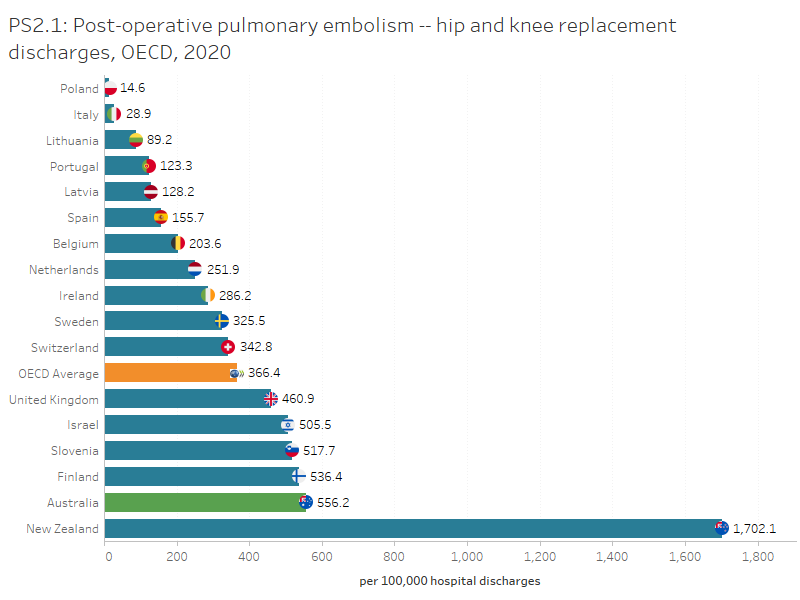
In Australia, the rate of PE after hip or knee replacement for people aged 15 and over was 556 per 100,000 hospitalisations in 2020, higher than the OECD average of 366 per 100,000 hospitalisations. Australia had the second highest rate of PE after hip or knee replacement among the OECD countries that submitted data for 2020 and Poland had the lowest rate with 15 per 100,000 hospitalisations.
In Australia, the rate has fluctuated over time in the past decade, ranging from 560 per 100,000 hospitalisations in 2013 to 472 per 100,000 hospitalisations in 2015.
Interactive PS2.1 below compares OECD countries that submitted data for 2020 for this indicator, while PM3.2 presents Australia’s 10-year trend for this indicator.
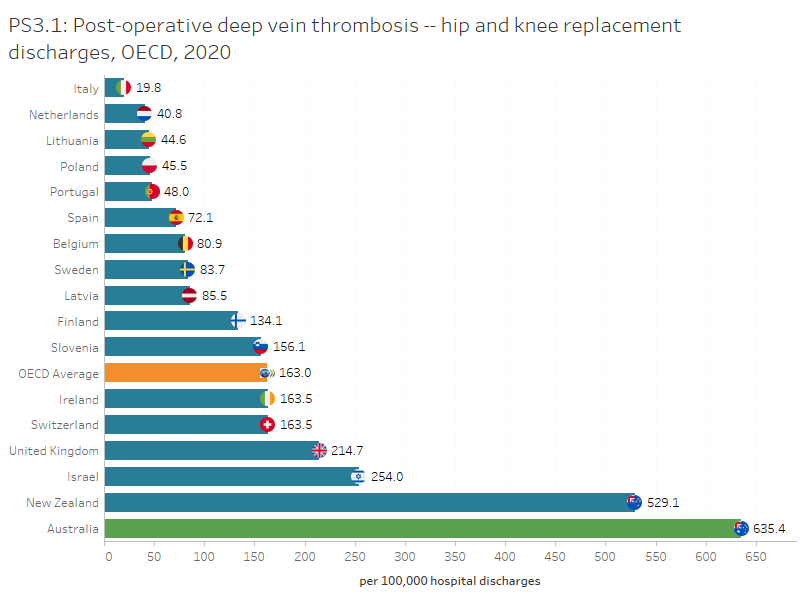
In Australia, the rate of DVT after hip and knee replacement for people aged 15 and over was 635 per 100,000 hospitalisations in 2020, higher than the OECD average of 163 per 100,000 hospitalisations. Australia had the highest rate of PE after hip or knee replacement among the OECD countries that submitted data for 2020 and Italy had the lowest rate with 20 per 100,000 hospitalisations.
In Australia, the rate has reduced over the past decade from 1,187 per 100,000 hospitalisations in 2011.
Interactive PS3.1 below compares OECD countries that submitted data for 2020 for this indicator, while PS3.2 presents Australia’s 10-year trend for this indicator.
Figures PS2.1 and PS2.2
PS2.1 presents OECD countries with data available for post-operative PE in hip and knee replacement hospitalisations indicator in 2020, which shows Australia had the highest rate. PS2.2 presents Australia’s 10-year trend for this indicator, which shows a fluctuating trend over time.
Figures PS3.1 and PS3.2
PS3.1 presents OECD countries with data available for post-operative DVT in hip and knee replacement hospitalisations indicator in 2020, which shows Australia had the highest rate. PS3.2 presents Australia’s 10-year trend for this indicator, which shows an overall decrease since 2010.
Refer to the Data tables for more information.
Post-operative sepsis – abdominal hospitalisations
Sepsis is the systematic response to an infection manifested by organ dysfunction, hypoperfusion or hypotension combined with one or more of the following: fever, tachypnoea, elevated white cell count (Antibiotic Expert Groups 2014). In many cases, post-operative sepsis can be prevented by prophylactic antibiotics, sterile surgical techniques, and good postoperative care (OECD 2017). The risk of sepsis following abdominal surgery is greater than following other surgical procedures (OECD 2015).
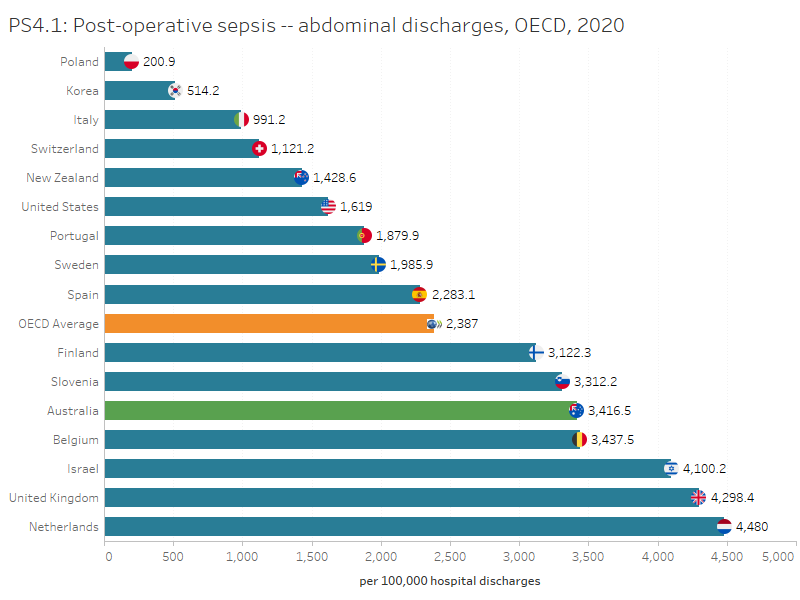
In Australia, the rate of post-operative sepsis for abdominal hospitalisations for people aged 15 was 3,416.5 per 100,000 hospitalisations in 2020, higher than the OECD average of 2,387 per 100,000 hospitalisations. Australia had one of the highest rates among OECD countries that submitted data, while Poland had the lowest rate (201 per 100,000 hospitalisations).
In Australia, the rate has increased from 2,641.5 per 100,000 hospitalisations in 2011 but has decreased from 4,190 per 100,000 hospitalisations in 2018.
Abdominopelvic procedure codes were required for the calculation of this indicator. The AIHW found that mapping was not straightforward in this instance as the ICD-9-CM codes supplied by the OECD did not map directly to the Australian Classification of Health Interventions (ACHI) code list used in Australia. The effect of this on the comparability of data is unknown.
Interactive P4.1 below compares OECD countries that submitted data for this indicator for 2020, while PS4.2 presents Australia’s 10-year trend for this indicator.
Figures PS4.1 and PS4.2
PS4.1 presents OECD countries with data available for post-operative sepsis in abdominal hospitalisations in 2020, which shows Australia had the 2nd highest rate. PS4.2 presents Australia’s 10-year trend for this indicator, which shows an overall increase since 2011.
Refer to the Data tables for more information.
Obstetric trauma with and without instrument
A woman’s safety during childbirth can be assessed by looking at potentially preventable, severe tearing of the perineum during vaginal delivery (OECD 2021). These types of tears cannot be completely prevented but can be reduced through appropriate labour management and high-quality obstetric care (OECD 2021).
Health at a glance 2023 recognised differences in data collection methods for obstetric trauma indicators among countries. According to the report, 'for Australia, Portugal, and the United States, data include women aged 15 and over, while in all other countries, the data pertain to women aged 18 years and above.'
The obstetric trauma with and without instrument indicators measure third and fourth degree tearing of the perineum during instrument-assisted (such as use of forceps or vacuum extraction) or non-assisted vaginal deliveries.
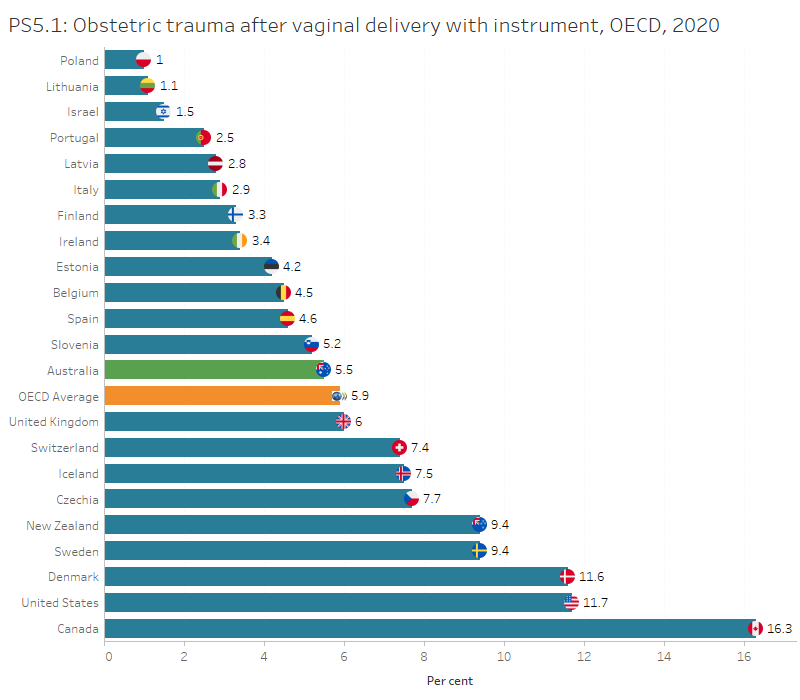
In Australia, the rate of obstetric trauma with instrument was 5.5 per 100 vaginal deliveries in 2020, lower than the OECD average of 5.9 per 100 vaginal deliveries. Among the OECD countries that submitted data for 2020 Poland had the lowest obstetric trauma rate (1 per 100 vaginal deliveries).
In Australia, the rate of obstetric trauma with instrument has reduced over the past decade from 7.5 per 100 vaginal deliveries in 2011.
Interactive PS5.1 below compares OECD countries that submitted data for 2020 for this indicator, while PS5.2 presents Australia’s 10-year trend for this indicator.
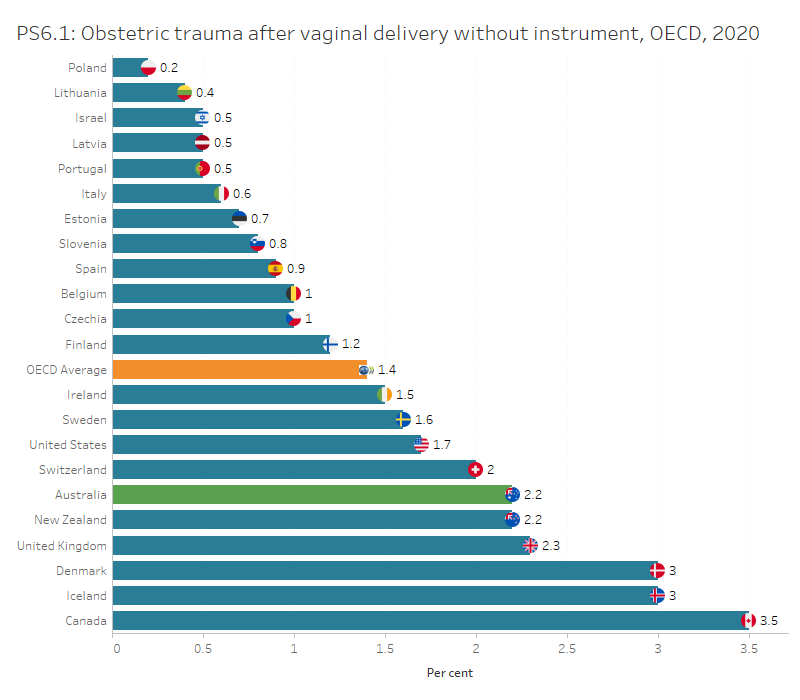
In Australia, the rate of obstetric trauma without instrument was 2.2 per 100 vaginal deliveries in 2020, higher than the OECD average of 1.4 per 100 vaginal deliveries. Among the OECD countries that submitted data for 2020 Poland had the lowest obstetric trauma rate (0.2 per 100 vaginal deliveries).
In Australia, the rate has remained relatively stable over the past decade.
Interactive PS6.1 below compares OECD countries that submitted data for 2020 for this indicator, while PS6.2 presents Australia’s 10-year trend for this indicator.
Figures PS5.1 and PS5.2
PS5.1 presents OECD countries with data available for obstetric trauma with instrument indicator in 2020, which shows Australia had a higher rate than the OECD average. PS5.2 presents Australia’s 10-year trend for this indicator, which shows an overall decrease since 2010.
Figures PS6.1 and PS6.2
PS6.1 presents OECD countries with data available for obstetric trauma without instrument indicator in 2020, which shows Australia had the 3rd highest rate. PS6.2 presents Australia’s 10-year trend for this indicator, which has remained between 2.3 and 2.5 per 100 vaginal deliveries since 2010.
ACSQHC (Australian Commission on Safety and Quality in Health Care) 2020. Australian sentinel events list. Version 2. Sydney: ACSQHC. Viewed 18 January 2024.
Antibiotic Expert Groups 2014. Therapeutic guidelines: antibiotic. Version 15. Melbourne: Therapeutic Guidelines Limited.
OECD 2013. Health at a glance 2013: OECD indicators. Paris: OECD.
OECD 2015. Health at a glance 2015: OECD indicators. Paris: OECD.
OECD 2017. Health at a glance 2017: OECD indicators. Paris: OECD.
OECD 2021. Health at a glance 2021: OECD indicators. Paris: OECD.
OECD 2023. Health at a glance 2023: OECD indicators. Paris: OECD.
NICE (National Institute for Health and Care Excellence) 2018. Venous thromboembolism in over 16s: reducing the risk of hospital-acquired deep vein thrombosis and pulmonary embolism. NG 89. London: NICE. Viewed 14 September 2021.
Yao L, Bae L and Yew WP 2013. Post-operative wound management. Australian Family Physician 42(12):867–70.