Compilation of health expenditure estimates
Overview
The HED, where the AIHW health expenditure data are collated and stored, is compiled each financial year. However, it takes approximately 15 to 18 months after the end of the reference year to receive, process, check and analyse the data, and release the HEA report.
Allocation of expenditure
The HED is structured to reflect the flow of funds in the health system (Figure 32), each column representing a funding source and the rows, the areas of expenditure (Table T1).
Derivation of expenditure estimates are based around the source of funding approach, whereby offsets are made to avoid double counting and to reflect the original source of funding.
This structure is reflected further in the estimates reported in the HEA, which presents health spending firstly by source of funds and secondly by area of expenditure.
State and territory level data
Data are disaggregated and reported at the state/territory level. Where the state/territory level data are not available in the source data, the expenditure estimates are allocated to the states and territories using allocation factors such as population or medical staffing proportions.
More detailed levels of geographical and demographical data (such as Statistical Area 3, data by age group, and data by socio-economic group) are not available in the HED. Such level of details might be available in AIHW’s Disease expenditure reports.
Offsets
Offsetting is the mechanism by which an adjustment is made for potential double counting of expenditure. By applying an offset, account is taken of circumstances where the same funds are spent more than once due to the way they flow in the health system. In these instances, a decision is required about which source the expenditure will be counted against. In the ANHA the source of funds approach is used to allocate expenditure to where the funds originated. The offsets are explained in detail throughout this chapter.
An example of an offset is that, as state and territory governments receive funding from the Australian Government, such as NHR funding and health-related NPPs, the spending is counted as components of spending by the Australian Government. The corresponding amounts are then deducted from state and territory governments’ gross expenditure to remove any double counting. Revenue that state and territory governments received from other sources (such as from DVA or non-government entities) are accounted for in a similar way.
Table T1: Health expenditure database structure and cell addresses, by source of funding (columns) by area of expenditure
View Table T1 Excel file (XLS 15KB)
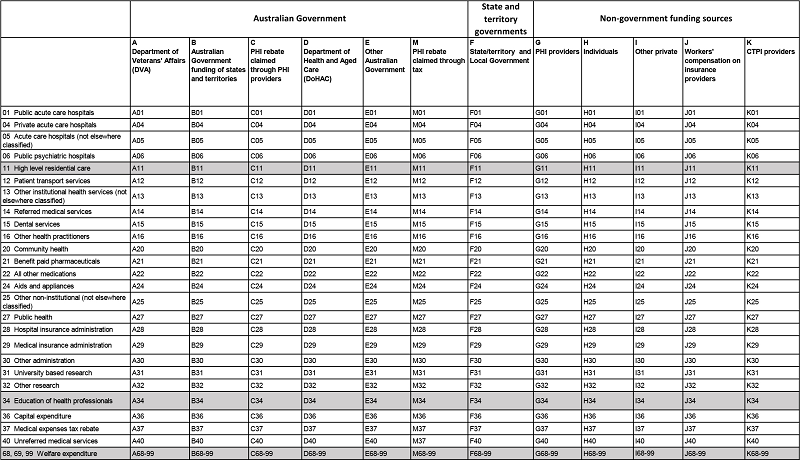
Notes:
High-level residential care (row 11) and Education of health professionals (row 34) are not currently considered to be in the scope of health expenditure. Rows 68, 69 and 99 are set up to take welfare expenditure. Expenditure for these categories is not included in the ANHA.
Rows 01, 05 and 06 are counted as public hospital services; rows 28, 29 and 30 combine to administration; while rows 31 and 32 are counted as research.