The burden of obesity
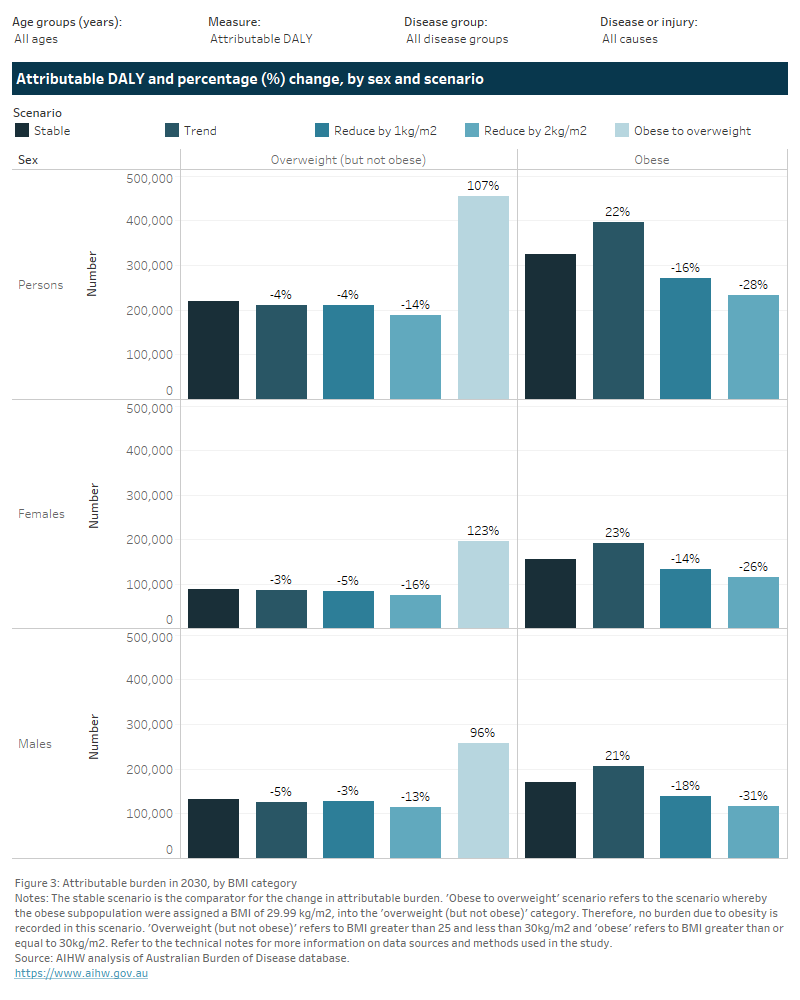
This figure presents two tabs of results on the changes in burden attributable to overweight (including obesity) in 2030 for each specific category of overweight (including obesity), by scenario relative to the stable scenario.
The first tab presents results by sex with two columns of results for each BMI category of overweight but not obese, and obesity. The second tab presents results by age.
Using the stable scenario as the baseline, if the population at risk reduced their BMI by 1 kg/m2, the burden attributable to obesity could be reduced from 324,000 to 272,000 DALY (52,100 fewer DALY) and from 13,400 to 11,500 deaths (1,900 fewer deaths) (Figure 3). This avoidable burden more than four times that of the potential reduction in burden attributable to living with overweight (but not obese) BMI (8,300 fewer DALY and 400 fewer deaths in the same scenario).
Compared with the stable scenario, the trend scenario shows an increase in burden attributable to obesity of 22% (or 72,000 DALY). Conversely, the trend scenario shows a decrease in burden attributable to the overweight (but not obese) category (a decrease of 4.2%, or 9,200 DALY). If current trends continued, 5.8% of total burden may be attributable to obesity compared with 4.8% in the stable scenario. This proportion decreases to 4% of total burden in the target scenario where BMI were to be reduced by 1 kg/m2.
The greater expected increase in 2030 for burden attributable to obesity compared with overweight (but not obese) BMI is seen across all age groups, and both males and females (trend scenario). However, the expected increase in obesity burden is greater among older age groups compared with younger age groups (40% increase in obesity burden for those aged 80 years and older compared with 4% for those under 40 years).
Across all age groups and sexes, the target scenarios indicate that greater improvements in burden occur through reductions to obesity-related burden compared with overweight (but not obese) burden.