Introduction
On this page:
An accessible and high-quality primary care sector is integral to Australia’s health care system. General practitioners (GPs) are the first point of contact for most Australians seeking health care (RACGP 2020a). In 2021–22, 90% of the population consulted GPs, underscoring their key role in health care delivery (AIHW 2023a). GPs are the most frequently accessed health professionals in Australia, and they are on the frontline in the battle against emerging health conditions such as Coronavirus disease 2019 (COVID-19) (RACGP 2021).
In 2021-22, nationally, there were 189 million GP attendances claimed through Medicare, with a Level B consultation (lasting less than 20 minutes) the most common type of attendance (AIHW 2022a). The number of Medicare-subsidised GP services per person increased with age, reaching its peak at 17.3 services per person for individuals aged 80 years and above, compared to 4.7 for the 0-14 years age group. There was a similar percentage of Medicare-subsided GP attendances for people living in metropolitan (90%) and regional (89.7%) Primary Health Network (PHN) areas (AIHW 2022a). Patient age and gender have an effect on the frequency of presentations, with females visiting their GP more than males, and older people visiting their GP more regularly than younger people (RACGP 2022).
The Practice Incentives Program (PIP) Quality Improvement (QI) Incentive is a payment to general practices for activities that support continuous data-driven quality improvement in patient outcomes and the delivery of best-practice care. General practices enrolled in the PIPQI Incentive commit to implementing continuous quality improvement activities that support them in their role of managing their patients’ health. They also commit to submitting nationally consistent, de-identified general practice data, against 10 key Improvement Measures that contribute to local, regional and national health outcomes (Department of Health 2019).
Purpose of the report
This is an annual data update on the 10 PIPQI measures. This report aims to provide nationally consistent, comparable data against specified measures that contribute to the assessment of needs, and to the improvement of regional and national health outcomes. The data, shared at the community level, and collected through the PIPQI Incentive, has the potential to inform primary health care providers on where care and services may be improved for clients, and within a population. For example, this report may be used to assist the understanding of what proportion of a population within a region may benefit from preventative measures to ensure effective management of a specified chronic disease, such as diabetes. This can help delay progression of the condition, improve quality of life, increase life expectancy and decrease the need for high cost interventions.
The improvement measures are intended to support a regional and national understanding of chronic disease management in areas of high need and are not designed to assess individual general practices or general practitioner performance. There are no set targets for the improvement measures.
The PIP Eligible Data Set
The de-identified data collected for the purposes of the PIPQI Incentive commenced on 1 August 2019, with participating general practices appointed as local data custodians, PHNs as regional data custodians, and the Australian Institute of Health and Welfare (AIHW) as the national data custodian of the PIPQI Eligible Data Set. For the specific roles and responsibilities of the local, regional, and national data custodians please refer to the Data Governance Framework (Department of Health 2021). The Incentive focuses on health service events that have taken place against 10 Quality Improvement Measures (QIMs) and is a payment to general practices for activities that support data-driven continuous quality improvement in patient outcomes and the delivery of best-practice care (Department of Health 2020a).
PHNs aim to enhance and connect primary health care within their region to achieve better health outcomes. Through their already established trust and working relationships with general practices, PHNs use the PIP Eligible Data Set to:
- work in partnership with local general practices to support quality improvement initiatives through reporting and feedback on managing general practice patient population, and
- perform needs assessments and plan service delivery at different levels, including PHN boundaries, local health districts, jurisdictional boundaries and at national level.
Data ecosystem
The health data ecosystem relies on high quality ‘electronic health records’ (EHRs) that play a crucial role in improving the provision of health care services and patient outcomes (AIHW 2022b). In Australia, general practices use various data management systems such as Clinical Information Systems (CISs) and extraction tools developed by various software providers to manage patient EHRs. The CISs are used by practices to electronically record administrative and clinical information. Extraction tools are developed by software providers to access de-identified data from CISs and generate reports to assist practices and PHNs with clinical audits, quality improvement activities, and research activities (RACGP 2020b).
Clinical information systems
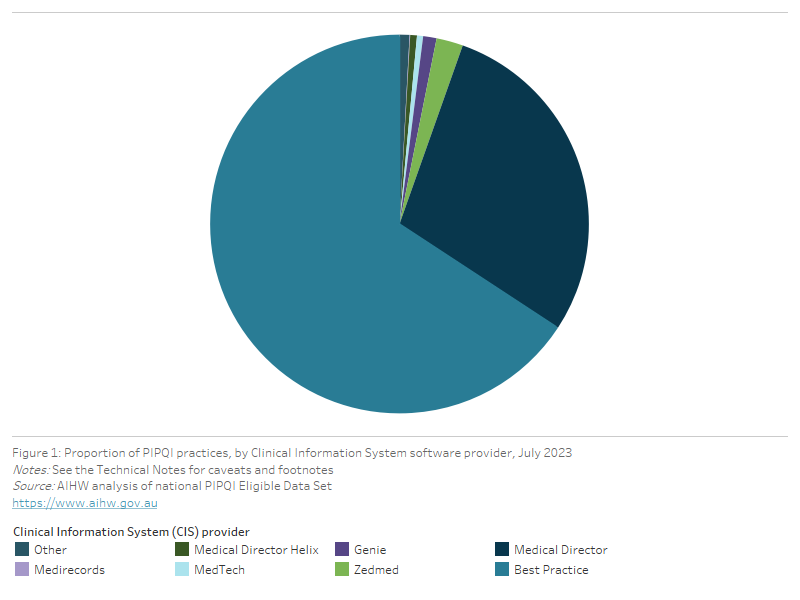
In July 2023, all 31 PHNs completed an AIHW survey to provide information on the CISs used by practices participating in the PIPQI Incentive. The most common CISs used were Best Practice (65.8%) and Medical Director Insights (28.8%), with a smaller proportion using other CISs (5.4%). The proportion of PIPQI practices using each CIS is shown in Figure 1.
Figure 1: Proportion of PIPQI practices, by Clinical Information System software provider, July 2023
This pie chart shows the proportion of PIPQI practices, by Clinical Information System software provider for July 2023
Data extraction tools
In the data submission period of July 2023, most PHNs used a single extraction tool, CAT Plus (74.2%), POLAR (16.1%), or Primary Sense (3.2%), to extract the PIPQI Eligible Data Set from practices. From 2022-23, some PHNs started using Primary Sense as their new extraction tool. As a result of this transition, more PHNs (6.5%) have started adopting a ‘hybrid’ extraction approach, combining two extraction tools to prepare and submit PIPQI data.
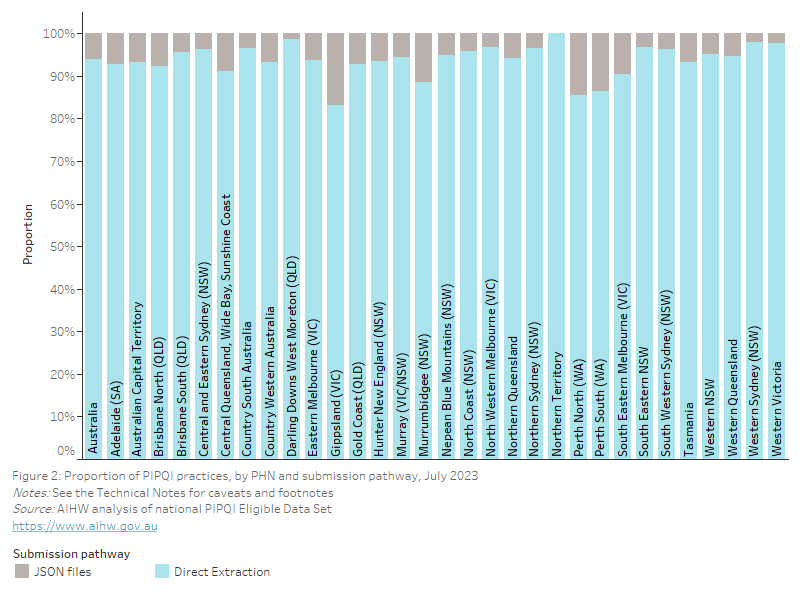
As local data custodians, general practices participating in the PIPQI Incentive provide data on service counts against each measure to their regional PHN data custodian. A practice generates an aggregate PIPQI report using either their CIS or an extraction tool (Department of Health 2020b) in accordance with the PIPQI Technical Specification v1.2 (Department of Health 2020c) and submits these data to their PHN using one of the following two submission pathways (Figure 2):
- Submission pathway 1: The majority of practices (93.9%, 5,531) used an extraction tool (CAT Plus, POLAR, Primary Sense) to generate and submit a PIPQI report. This approach is also referred to as ‘direct extraction’.
- Submission pathway 2: Some practices instead used their CIS to generate a PIPQI report as a JSON (JavaScript Object Notation) file which they submit to their PHN (Department of Health 2020c). There are also some practices that used the CAT Plus extraction tool to generate PIPQI JSON files because their CIS lacked this functionality. In contrast to previous years, there were more practices (6.1%, 361) that submitted data as JSON files due to incompatibility between the practice CIS and extraction tools.
Figure 2: Proportion of PIPQI practices, by PHN and submission pathway, July 2023
This bar chart shows the proportion of PIPQI practices, by PHN and submission pathway for July 2023
Data collection
The AIHW obtained Ethics Committee approval on 15 July 2021 for the establishment of this data collection. As of July 2023, 5,531 general practices across 31 PHNs contributed to the national aggregate PIPQI data.
Data from clients who opted-out from sharing de-identified data between practices and PHNs were not extracted and are not included in this report. A review commissioned by the Department of Health found that the data security controls in place during the collection, use and storage are appropriate to protect de-identified data from misuse, interference, and loss (Department of Health 2020d).
Data quality
Each PHN collated and aggregated PIPQI data extracts from general practices in accordance with the definitions of the 10 QIMs and the permissions outlined in the Data Governance Framework (p15, Table 1, Department of Health 2021). Aggregate data files were validated and submitted by PHNs to the AIHW on a quarterly basis, using a secure web-based data submission platform.
The AIHW also validated the aggregate data received from PHNs using a series of defined rules to identify and resolve data quality issues. The latest data were compared with the data from the previous quarters and other variance metrics for further analysis. In cases where the data failed to meet any of the validation rules, the respective PHN was asked to review and resubmit the data. Additionally, the AIHW engaged with software providers to collaboratively resolve data quality issues arising from CISs or extraction tools. Any inconsistencies and caveats are documented in the Technical notes section.
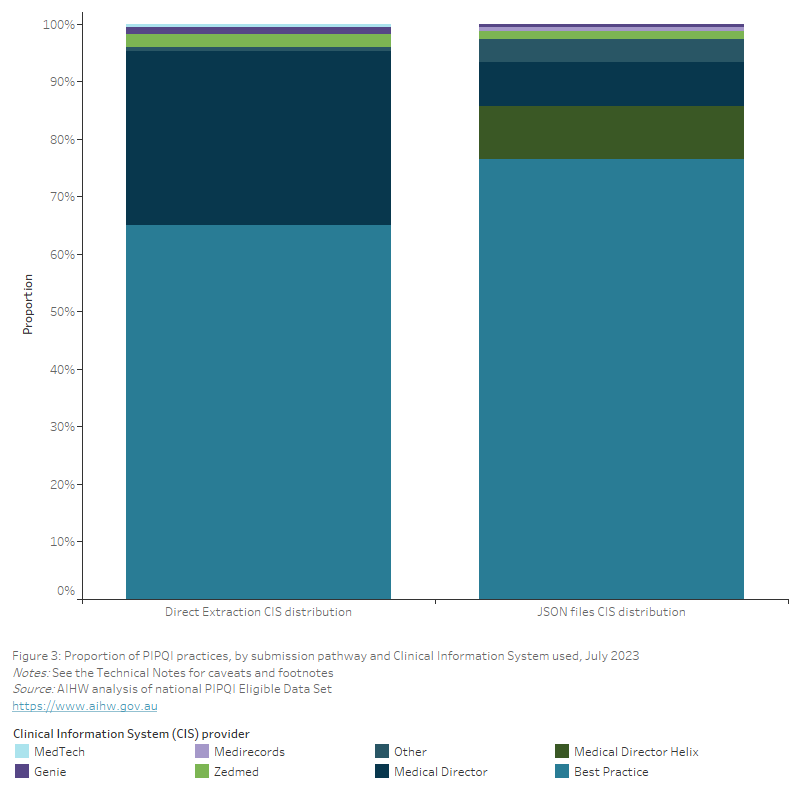
In July 2023, 4 PHNs combined excluded a total of 22 data files generated by the Primary Sense tool from national reporting due to technical issues arising from a ‘hybrid’ extraction arrangement while transitioning from one extraction tool to another. Therefore, the extraction tool results may underestimate the use of Primary Sense in PIPQI reporting. There was also 1 PHN that excluded 1 CAT Plus generated data file due to technical issues. For further information, please refer to the footnotes of the relevant visualisations. Additionally, all 361 JSON files were excluded for reporting purposes due to ongoing data quality issues affecting multiple QIMs. Of the excluded JSON files, 276 were generated using Best Practice, 61 using Medical Director, 6 using PrimaryClinic Medical, and 3 using MediRecords (Figure 3). The remaining 15 JSON files that were excluded were generated using an extraction tool because the CISs used by the practices submitting these files did not have the required functionality.
Figure 3: Proportion of PIPQI practices, by submission pathway and Clinical Information System used, July 2023
This bar chart shows the proportion of PIPQI practices, by submission pathway and Clinical Information System used for July 2023
To mitigate inconsistencies caused by ongoing data quality issues in the JSON files, PHNs have also been submitting data files to the AIHW which were generated exclusively by direct extraction since January 2023. Consequently, the QIM-specific time trend visualisations presented in this report only display directly extracted data from January 2023 to July 2023. This approach ensures that data of poor quality are excluded, leading to a more accurate representation of the data and trends.
The AIHW compiled the data received from PHNs and generated national estimates based on the supplied numerators and denominators for each QIM. The underlying data used for this report are supplied in the Practice Incentives Program Quality Improvement Measures – Data Tables for download.
The AIHW observed differences in the aggregate data due to different interpretations of the technical specifications and coding of the QIMs by CIS and extraction tool providers. The resulting differences in the QIM proportions by extraction tool are visualised for each measure in this report. For further description of PIPQI data quality and subsequent actions to resolve data issues, please refer to the Technical notes.
Regular clients
PIPQI data submitted by PHNs only include ‘active’ or ‘regular’ clients – an individual who has visited a practice 3 or more times in the 2 years prior to the date of data extraction and whose service events were eligible for an MBS rebate. This is consistent with the RACGP definition of an active patient/client (RACGP 2020c). Therefore, clients who visited a practice less than this amount are not included in this report. Note that those 3 visits could be at any time during the 2 years and do not necessarily mean that attendance at a practice has been recent.
Telehealth played a very important role in maintaining patient care during the COVID-19 pandemic (AIHW 2022c). Temporary telehealth MBS item numbers were made available from 13 March 2020 in response to the COVID-19 pandemic (Department of Health 2022). In 2020, 22% of General Practice visits were conducted via telehealth, and 20% in 2021 (AIHW 2022c). However, these temporary MBS items were not included in the scope of MBS items used to calculate the Standardised Whole Patient Equivalent (SWPE) for the purposes of payment calculations under the Practice Incentives program (PIP), including the payments for the PIP Quality Improvement Incentive, until January 2022 (Department of Health 2022). This means that telehealth consultations received during this period were not counted towards the RACGP definition of a regular client (patient) who visited a particular primary health care provider three or more times in the last two years. Therefore, the actual aggregate QIM specific regular client cohort and proportions may be under-represented both nationally and in a PHN for that duration. Readers of this report should take these factors into consideration when interpreting the findings.
A range of public health interventions were put in place to help contain the spread of the virus that causes COVID-19. These included border controls; closure of non-essential businesses; work-from-home orders; school closures; density limits within businesses and workplaces; stay-at-home orders; mandated mask use; and test, trace, isolation and quarantine measures (AIHW 2022c). As many GPs and their patients used telehealth consults over face-to-face visits during the COVID-19 pandemic, there would have been fewer opportunities to take physical measures such as blood pressure, weight and height, and pathology testing thus impacting the overall regular client numbers for the related PIPQI measures. It is difficult to quantify the impacts of COVID-19 on the clients visiting general practices due to several factors including lockdowns, client health seeking behaviour, redistribution of practice resources, introduction and recalibration of telehealth consultations, and service re-orientation to focus on provision of vaccination only (AIHW 2022c). A Digital Health Cooperative Research Centre and Macquarie University report from 800 general practices in select Victorian and NSW PHNs identified an increased uptake of telehealth services throughout the pandemic, which may reflect varied public health responses to the COVID-19 pandemic in those jurisdictions (Hardie et al. 2021).
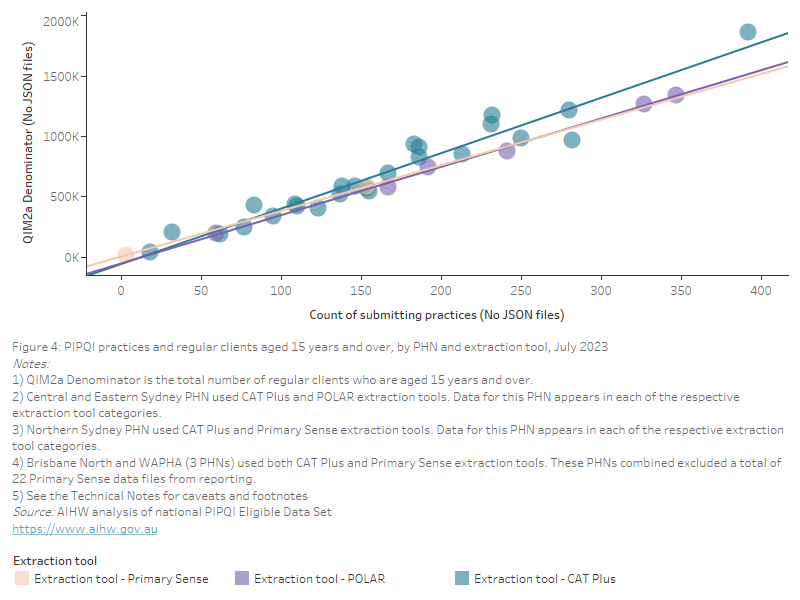
As some clients actively attend more than one practice, including across more than one PHN region, the aggregated totals will report on these individuals more than once. For example, some people may attend one practice near their home or workplace while another near a holiday home. These totals do not represent the total resident population, or the total number of individuals who actively attend practices, or the prevalence of cohorts or conditions, or the percentage of the total population that attends practices. This may impact some PHN regions more than others due to the high prevalence of holiday homes. Figure 4 below presents an estimated count of regular clients aged 15 years and older who visited PIPQI practices during July 2023 in each PHN broken down by the extraction tool used. The estimates are based on the QIM2a denominator.
Figure 4: PIPQI practices and regular clients aged 15 years and over, by PHN and extraction tool, July 2023
This scatterplot shows the number of PIPQI practices and regular clients aged 15 years and over, by PHN and extraction tool for July 2023
There are differences in the types of visits that are counted towards the definition of a regular client across CISs and extraction tools which may impact the proportions reported for each QIM. The AIHW is collaborating with these software providers to align the interpretation of the QIMs with the technical specifications.
As there are a variety of counting rules to distinguish clinical and non-clinical visits in CISs and extraction tools, figures in this report should be interpreted with these caveats in mind. For further detail, please refer to the Technical notes.
Interpreting PIPQI data
Results included in this report should be interpreted with care, taking into consideration the points raised above. In addition, it should be noted that this report provides information on a specific set of items for PIPQI and does not provide information about the complete range of care that is provided to a client.
Where data are presented as a time series, the results represent national point-in-time proportions of cohorts with a recorded result at each quarter.
This data should be interpreted in conjunction with other administrative and survey data collections where the data from these client-provider interactions are captured, for example, Medicare Benefits Schedule (MBS), the Australian Immunisation Register (AIR), the National Diabetes Service Scheme (NDSS) Register, the Australasian Paediatric Endocrine Groups (APEG) state and territory registers, the National Cancer Screening Register (NCSR), the National Health Survey, and State and Territory Health surveys.
For a full list of caveats and footnotes, please refer to the Technical notes.
PHN Boundaries and Residential Population
In 2015, PHNs were established with the key objectives of increasing the efficiency and effectiveness of medical services for patients, particularly those at risk of poor health outcomes, and improving coordination of care to ensure patients receive the right care in the right place at the right time (Department of Health 2023). Where possible, boundaries of the PHNs align with Local Hospital Networks (LHNs) or equivalents, or cluster of LHNs, to facilitate collaborative working relationships and reduce duplication of effort. The analysis of data at a regional level allows for the planning, commissioning and provisioning of health services based on the local needs assessments of the community.
There are 31 PHNs that cover the whole of Australia and, in determining boundaries, a number of factors were taken into account, including diverse population size and future projected population growth, LHN alignment, State and Territory borders, patient flows and administrative efficiencies (Department of Health 2023).
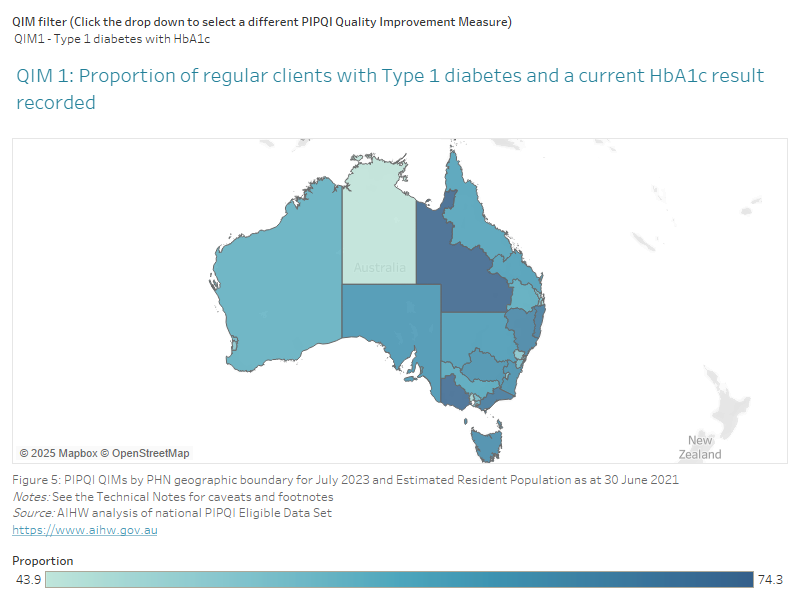
PHNs vary considerably in geographical size and residential population at a community level (Department of Health 2021). In 2021, PHN population by usual residence varied from 63,615 to 1,849,932 people (ABS 2021a). Some residents of PHNs may seek health services provided by other adjacent or non-adjacent PHNs. Across PHNs, the percentage of adults (>15 years of age) who visited a general practice in the previous 12 months in 2019–20 varied from 78.6% to 87.1% (AIHW 2021a). Please see Figure 5 below for an overview of the PIPQI QIMs and Estimated Resident Population by PHN geographic boundaries.
Figure 5: PIPQI QIMs by PHN geographic boundary for July 2023 and Estimated Resident Population as at 30 June 2021
This map shows the PIPQI QIMs by PHN geographic boundary for July 2023 and Estimated Resident Population as at 30 June 2021
For estimated resident population in each PHN, please refer to the data tables provided in the Practice Incentives Program Quality Improvement Measures - Data tables for download.
ABS (Australian Bureau of Statistics) (2021a) Regional population by age and sex as at 30 June 2021 (preliminary rebased), ABS, Canberra, accessed 2 August 2023. Obtained by the AIHW from the ABS via data request on 09/09/2022
AIHW (Australian Institute of Health and Welfare) (2021a) Patient experiences in Australia by small geographic areas in 2019–20, AIHW, Canberra, accessed 1 August 2023.
AIHW (2022a) Medicare-subsidised GP, allied health and specialist health care across local areas: 2021–22, AIHW, Canberra, accessed 04 August 2023.
AIHW (2022b) Digital health, AIHW, Canberra, accessed 1 August 2023.
AIHW (2022c) Australia’s health 2022: data insights, catalogue number AUS 240, Australia’s health series number 18, AIHW, Canberra, accessed 1 August 2023.
AIHW (2023a) General practice, allied health and other primary care services, AIHW, Canberra, accessed 1 August 2023.
Department of Health (2019) PIPQI Incentive guidance, Department of Health, Canberra, accessed 3 August 2023.
Department of Health (2020a) Practice Incentives Program Quality Improvement Measures User Guide for General Practices, Department of Health, Canberra, accessed 10 July 2023.
Department of Health (2020b) Practice Incentives Program Quality Improvement Measures User Guide for Primary Health Networks, Department of Health, Canberra, accessed 6 July 2023.
Department of Health (2020c) PIPQI Improvement Measures Technical Specification v1.2 22102020, Department of Health, Canberra, accessed 2 August 2023.
Department of Health (2020d) Practice Incentives Program Quality Improvement Incentive Data Privacy and Security Review: Summary and Recommendations, Department of Health, Canberra, accessed 2 August 2023.
Department of Health (2021) PIP Eligible Data Set Data Governance Framework, Department of Health, Canberra, accessed 2 August 2023.
Department of Health (2022) COVID-19 Temporary MBS Telehealth Services: Factsheets on the use of the temporary MBS telehealth and phone consultation item numbers, Department of Health, Canberra, accessed 2 August 2023.
Department of Health (2023) Primary Health Networks, Department of Health, Canberra, accessed 2 August 2023.
Hardie R-A, Sezgin G, Dai Z, Wabe N, Georgiou A (2021) Socioeconomic and demographic comparisons in the uptake of telehealth services during COVID-19. COVID-19 General Practice Snapshot, Issue 2: 22, Macquarie University, Sydney, accessed 1 August 2023.
RACGP (The Royal Australian College of General Practitioners) (2020a) The role of specialist GPs: Position Statement October 2020, RACGP, East Melbourne, Victoria, accessed 2 August 2023.
RACGP (2020b) Practice Incentives Program Quality Improvement Incentive (PIPQI) fact sheet, RACGP, East Melbourne, Victoria, accessed 6 July 2023.
RACGP (2020c) Standards for general practices, 5th edition, RACGP, East Melbourne, Victoria, accessed 2 August 2023.
RACGP (2021) General Practice: Health of the Nation 2021, RACGP, East Melbourne, Victoria, accessed 2 August 2023.
RACGP (2022) General Practice: Health of the Nation 2022, RACGP, East Melbourne, Victoria, accessed 7 August 2023.