Australia's youth:
Mental illness
Web article
Last updated:
Topic: Children & youth
Part of Australia's youth
Citation
AIHW
Australian Institute of Health and Welfare (2021) Mental illness, AIHW, Australian Government, accessed 26 April 2024.
APA
Australian Institute of Health and Welfare. (2021). Mental illness. Retrieved from https://pp.aihw.gov.au/reports/children-youth/mental-illness
MLA
Mental illness. Australian Institute of Health and Welfare, 25 June 2021, https://pp.aihw.gov.au/reports/children-youth/mental-illness
Vancouver
Australian Institute of Health and Welfare. Mental illness [Internet]. Canberra: Australian Institute of Health and Welfare, 2021 [cited 2024 Apr. 26]. Available from: https://pp.aihw.gov.au/reports/children-youth/mental-illness
Harvard
Australian Institute of Health and Welfare (AIHW) 2021, Mental illness, viewed 26 April 2024, https://pp.aihw.gov.au/reports/children-youth/mental-illness
Key findings
- In 2013–14, 1 in 5 (20%) young people aged 11–17 had either high or very high levels of psychological distress (13% and 6.6%, respectively).
- In 2017–18, an estimated 339,000 young people aged 18–24 (15%) experienced high or very high levels of psychological distress.
- In 2013–14, an estimated 245,000 young people aged 12–17 (14%) experienced a mental disorder, with males more commonly affected than females (16% compared with 13%).
- In 2019, there were 461 deaths by suicide among young people aged 15–24, a rate of 14 per 100,000 young people.
Most young people in Australia are happy, feel positive about the future and are satisfied with their lives overall (see also Subjective wellbeing). However, some young people suffer poor mental health.
Mental health is a state of wellbeing in which an individual realises their own abilities, can cope with the normal stresses of life, can work productively and can contribute to their community. Poor mental health can impact on the potential of young people to live fulfilling and productive lives (WHO 2018).
Psychological distress is an individual’s overall level of psychological strain or pain. It is evidenced by psychological states such as depression and anxiety (AIHW 2011). The Kessler 10 Psychological Distress Scale (K10) has been shown to be highly correlated with the presence of depressive or anxiety disorders (Lawrence et al. 2015).
Mental illnesses (also referred to as mental health disorders) are diagnosable health conditions. They are health problems that affect how a person feels, thinks, behaves and interacts with others (DoH 2007). Mental illness can vary in severity and duration and may be episodic (AIHW 2018). However, most mental disorders can be effectively treated, and earlier treatment leads to better outcomes (DoH 2007).
The National Children’s Mental Health and Wellbeing Strategy is being developed to ensure that mental illnesses are diagnosed and treated early to prevent lifelong disability (NMHC 2019). A range of mental health services are available in Australia; for detailed information, see Mental health services in Australia.
Poor mental health can be associated with suicidality (that is, suicidal ideation, suicide plans and suicide attempts). However, while suicidality is common in people with mental disorders, it is not confined to this group (Slade et al. 2009 in AIHW 2018). In 2015, suicide and self-inflicted injury was the leading cause of the total burden of disease for young people aged 15–24, followed by anxiety disorders and depressive disorders. Alcohol use disorders was the fifth leading cause (AIHW 2019) see Burden of disease.
Mental health concerns and rates of deaths by suicide among young people were raised as key challenges by young people during consultations by the Youth Taskforce in 2019 to assist in the development of the National Youth Policy Framework (the Framework) (DoH 2020).
Box 1: Data sources, definitions and limitations
Psychological distress
Data on psychological distress are sourced from Young Minds Matter survey (for ages 11–17) and the ABS National Health Survey 2017–18 (for ages 18–24). Both surveys use the K10. This scale consists of 10 questions about negative emotional states in the past 30 days (see ABS 2018b and Lawrence et al. 2015 for more details).
Mental illness
The latest national data on mental illness for young people aged 11–17 are sourced from the Second Australian Child and Adolescent Survey of Mental Health and Wellbeing (also known as, and hereafter referred to as, the Young Minds Matter survey), and the Young Minds Matter Survey Results Query Tool). This household survey was conducted in 2013–14 by the Telethon Kids Institute at the University of Western Australia, in partnership with Roy Morgan Research. A total of 6,310 parents and carers responded, as well as 2,967 young people aged 11–17 in those households where parents or carers had given permission for them to respond and also completed a questionnaire. Data relating to young people aged 12–17 in this section are based on parent and/or carer reported data; some self-reported data are included for young people aged 11–17.
Young people with mental health disorders are those who meet the criteria for a medical diagnosis of a mental disorder within the 12 months before the survey. Diagnoses were based on the DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, 4th edition).
Data on mental disorders for young people aged 16–24 are sourced from the Australian Bureau of Statistics (ABS) National Survey of Mental Health and Wellbeing 2007. The survey based its classification of mental disorders on existing diagnostic criteria to estimate prevalence (ABS 2008). Data on the prevalence of mental disorders from the 2007 survey are due to be updated from 2020–21 as part of the Intergenerational Health and Mental Health Study. This will consist of 4 surveys over 3 years. The survey will also include data on the impact of mental and behavioural and other chronic health conditions on Australians, and lived experiences of suicide (ABS 2021).
Self-reported mental and behavioural conditions
Data on mental and behavioural conditions for ages 15 to 24 are sourced from the ABS National Health Survey 2017–18, which provides data on a range of health conditions including mental and behavioural disorders. Estimates are based on self‑reported data, and record a participant as having a mental or behavioural condition during the collection period only if it was also reported as long term (that is, had lasted, or was expected to last, a minimum of 6 months) (ABS 2018b) (see also Technical notes).
Self-harm
Data on hospitalised injury cases for self-harm are sourced from the AIHW National Hospital Morbidity Database (NHMD). The NHMD is a collection of episode-level records from admitted patient morbidity data collection systems in Australian hospitals. It includes records for all episodes of admitted patient care from essentially all public and private hospitals in Australia.
Deaths by suicide
Data on deaths by suicide are sourced from the Australian Bureau of Statistics (ABS) Causes of Death. These data include information about causes of death and other characteristics of the person, such as sex, age at death, area of usual residence and Indigenous status. The cause of death data are compiled and coded by the ABS to the International Statistical Classification of Diseases and Related Health Problems (ICD).
The information is provided to the ABS by state and territory Registrars of Births, Deaths and Marriages for coding and compilation into aggregate statistics. Generally, most deaths due to external causes will be referred to a coroner for investigation; this includes those deaths that are possible instances of intentional self-harm (death by suicide) (ABS 2019). In addition, the ABS supplements these data with information from the National Coronial Information System (NCIS).
Ambulance attendances
Data on ambulance attendances are sourced from the National Ambulance Surveillance System (NASS), a partnership between Turning Point, Monash University and jurisdictional ambulance services across Australia (AIHW 2020b). The NASS collates and codes monthly ambulance attendances data for participating states and territories for self-harm behaviours (suicidal ideation, suicide attempt, death by suicide, self-injury) and mental health (AIHW 2020b).
Data limitations for deaths by suicide, intentional self-harm or suicidal ideation
This section draws on mortality, hospitals and survey data. Data from emergency departments (EDs) or primary health-care services cannot currently capture those presenting with intentional self-harm or suicidal ideation in most jurisdictions. Many others will not seek medical treatment.
The Australian Institute of Health and Welfare (AIHW) is currently working with key stakeholders, including the Mental Health Information Strategy Standing Committee and ED data custodians, to develop a nationally consistent method to identify and collect data on suicide-related ED presentations (AIHW 2020a).
A further difficulty in determining the incidence of suicidal and self-harming behaviours is that the International Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) used to code cause of death data and International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification (ICD-10-AM) used to code hospital admission data cannot distinguish between the suicidal and non-suicidal intent of self-harm (AIHW 2020a).
In this report, deaths by suicide are presented according to year of registration, not necessarily the year in which the death occurred.
How many young people experience psychological distress?
As this section draws on different data sources for different age groups, data for age groups 11–17 and 18–24 are reported separately.
In 2013–14, based on self-reported data in the Young Minds Matter survey among young people aged 11–17:
- 1 in 5 (20%) had either high or very high levels of psychological distress (13% and 6.6%, respectively)
- a higher proportion of females had high or very high levels of psychological distress (16% and 9.5%, respectively) compared with males (10% and 4.0%)
- a higher proportion of those aged 16–17 had high or very high levels of psychological distress (11% and 16%) compared with those aged 11–15 (4.8% and 12%) (Figure 1).
Figure 1: Level of psychological distress among 11–17 year olds, by age group and sex, 2013–14
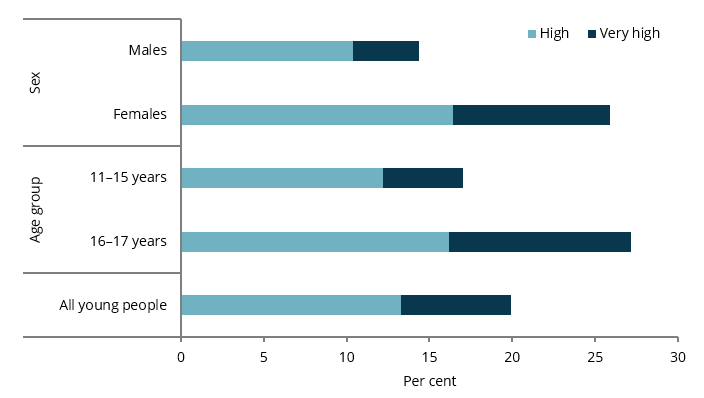
Chart: AIHW.
Source: AIHW analysis of the Young Minds Matter Survey Results Query Tool.
In 2017–18, based on self-reported data in the ABS National Health Survey among young people aged 18–24:
- an estimated 15% (or 339,000) had high or very high levels of psychological distress – 29% reported moderate levels and 49% had low levels
- a higher proportion of females than males reported high or very high levels of psychological distress (18% and 12%, respectively).
Has there been a change over time?
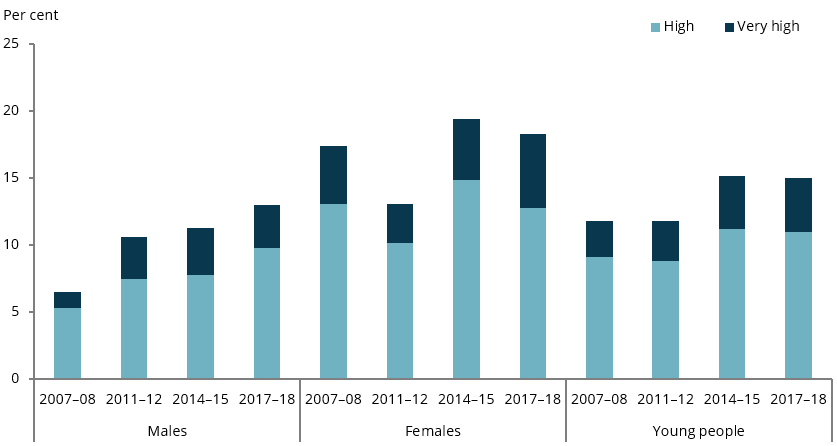
Among young people aged 18–24, the rate of high or very high psychological distress increased from 12% to 15% between 2011–12 and 2014–15. However, there was little change between 2014–15 and 2017–18.
For females aged 18–24, the rate of high or very high psychological distress also rose between 2011–12 and 2014–15, from 13% to 20%. However, there was little change between 2014–15 and 2017–18 (Figure 2).
Levels of psychological distress for females aged 18–24 were higher than all other age groups in 2014–15, and higher than those aged 35–44, 65–74 and 75 years and over in 2017–18 (ABS 2015, ABS 2018a).
Figure 2: Psychological distress among 18–24 year olds, by sex, 2011–12 to 2017–18
Note: The data for females 2011–12 have a relative standard error (RSE) of 25% to 50% and should be treated with caution.
Chart: AIHW.
Sources: ABS 2012, 2015, 2018a.
How many young people have mental illness?
In 2013–14, based on information collected from parents/carers in the Young Minds Matter survey, among young people aged 12–17:
- an estimated 245,000 (around 14%) experienced a mental disorder in the 12 months before the survey, with a higher proportion of males than females (16% compared with 13%) (AIHW analysis of the Young Minds Matter Survey Results Query Tool; Lawrence et al. 2015)
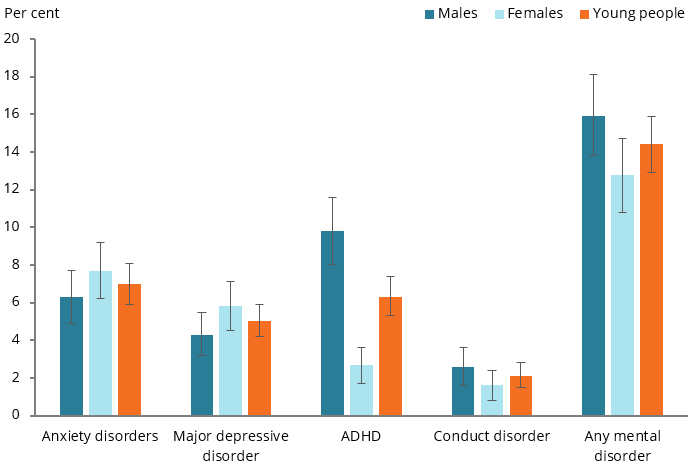
- anxiety and attention-deficit/hyperactivity disorder (ADHD) were the most common disorders (7.0% and 6.3%, respectively). Anxiety was the most common disorder among girls (7.7%) and ADHD the most common disorder among boys (9.8%) (Figure 3).
In relation to major depressive disorder, the survey collected information from young people (aged 11–17) themselves, as well as information from their parents/carers. The prevalence of major depressive order among 11–17 year olds was higher (7.7%) based on adolescent-reported information than on information reported by parents/carers (4.7%) (Lawrence et al. 2015). When considering information provided by parents/carers together with information provided by young people themselves, the prevalence was higher again, with 11% of 11–17 year olds meeting the diagnostic criteria for major depressive disorder (Lawrence et al. 2015).
Young people rated how much their parents or carers knew about how they were feeling. The proportion who reported that their parent/carers know ‘not at all’ how they are feeling was:
- 7.4% among those who did not have major depressive disorder
- 15% among those where both the parent/carer report and young person report indicated that the young person had major depressive disorder
- 30% among those where only the young person report indicated major depressive disorder (Lawrence et al. 2015).
Figure 3: Mental disorders among 12–17 year olds(a), by sex, 2013–14
(a) In the 12 months before the survey.
Note: Findings are based on parent and/or carer-reported data for young people.
Chart: AIHW.
Source: AIHW analysis of the Young Minds Matter Survey Results Query Tool.
Among young people aged 12–17 with mental disorders, the severity of the impact was:
- mild for more than 4 in 10 (44%) young people
- moderate for more than 3 in 10 (33%) young people
- severe for more than 2 in 10 (23%) young people.
There was little difference in the proportions of males and females at each level of impact (Lawrence et al. 2015). However, the proportion of 12–17 year olds with severe impact was almost 3 times as high as that for 4–11 year olds (23% and 8.2%, respectively) (Lawrence et al. 2015).
In 2007, based on the ABS 2007 National Survey of Mental Health and Wellbeing, among young people aged 16–24:
- an estimated 1 in 4 (26% or 671,100) experienced at least 1 mental disorder in the preceding 12 months
- anxiety disorders were the most commonly reported disorder for all young people overall (15%) followed by substance use disorders (13%) and affective disorders (6%). For more information, see Young Australians: their health and wellbeing 2011.
Data on the prevalence of mental disorders from the 2007 survey are due to be updated from 2020–21 as part of the Intergenerational Health and Mental Health Study (see Box 1 for details).
More recent data on self-reported long-term mental and behavioural conditions is available from the National Health Survey 2017–18. Results show that among young people aged 15–24:
- 26% reported having any long-term mental or behavioural condition, with the proportion higher among females (30%) than males (21%) (ABS 2018a)
- the most common conditions were anxiety disorders/feeling anxious, nervous or tense (17%) and depression/feeling depressed (12%) (ABS 2018a).
Between 2014–15 and 2017–18, the proportion of young people reporting having any long-term mental or behavioural condition increased from 19% to 26% (ABS 2018a) (see also Technical notes regarding comparisons over time).
Has there been a change over time?
Between 1998 and 2013–14, comparisons of 3 disorders (major depressive disorder, ADHD and conduct disorder) reported in the Young Minds Matters surveys showed that among young people aged 12–17, the proportion:
- of those who had any of the 3 disorders remained stable (10% in 1998 and 11% in 2013–14)
- with major depressive disorder increased from 2.9% to 5.0%
- with ADHD was similar (7.1% in 1998 and 6.3% in 2013–14).
- with conduct disorder showed little change (2.2% to 2.1%) (Lawrence et al. 2015).
Box 2: How many young people use mental health services?
A wide variety of support services are available to assist young people with emotional and behavioural problems.
While comprising 12% of the Australian population, in 2019–20, young people aged 12–24 made up 22% (587,000) of all people receiving Medicare-subsidised services specific to mental health, and accounted for:
- 20% (85,800) of people receiving services from psychiatrists
- 22% (496,000) of people receiving services from general practitioners
- 23% (127,000) of people receiving services from clinical psychologists
- 24% (176,000) of people receiving services from other psychologists
- 24% (27,600) of people receiving services from other allied health providers (AIHW 2021b).
In 2019–20, young people aged 12–24 also made up 25% (76,100) of ED presentations for mental-health-related care (AIHW 2021c).
In 2018–19, young people aged 12–24 accounted for:
- 28% (124,900) of community mental health care service patients (AIHW 2021a)
- 22% (4,100) of same-day admitted mental health-related separations from public hospitals with specialised psychiatric care and 17% (6,800) of those without specialised psychiatric care (AIHW 2021e)
- 20% (34,200) of overnight admitted mental health-related hospital separations from public hospitals with specialised psychiatric care and 11% (10,600) of those without specialised psychiatric care (AIHW 2021d).
For more information on mental health service use in Australia, see Mental health services in Australia.
Monitoring data on deaths by suicide and self-harm
Please carefully consider your needs when reading the following information about suicide and self-harm. If this report raises any issues for you, these services can help:
- Lifeline 13 11 14
- Suicide Call Back Service 1300 659 467
- Kids Helpline 1800 55 1800
- MensLine Australia 1300 78 99 78
- Beyond Blue 1300 22 4636.
Crisis support services can be reached 24 hours a day.
The AIHW supports the use of the Mindframe guidelines on responsible, accurate and safe reporting of suicide and self-harm. Please consider these guidelines when communicating about suicide and self-harm.
How many young people self-harm and engage in suicidal behaviour?
Based on self-reported data in the Young Minds Matter survey, in 2013–14, among young people aged 12–17:
- around 1 in 10 (11% or an estimated 186,000) reported ever having deliberately injured themselves. Around 7.5% reported that they preferred not to say, indicating that the proportion may be higher. The proportion was:
- almost twice as high among females as males (15% compared with 6.8%)
- almost twice as high among those aged 16–17 (16%) as among those aged 12–15 (8.2%)
- 5.9% of young people (or 100,000) had self-harmed 4 or more times over their lifetime, with the proportion:
- more than 3 times as high for females (9.2%) as males (2.8%)
- 2.6 times as high for those aged 16–17 (9.8%) as for those aged 12–15 (3.8%)
- 8.0% of young people (or 137,000) had self-harmed in the past 12 months, with the proportion:
- more than 3 times as high for females (12%) as males (4.0%)
- nearly twice as high for those aged 16–17 (12%) as for those aged 12–15 (6.2%)
- around 128,000 or 7.5% had seriously considered attempting suicide in the previous 12 months. The proportion was over twice as high for females as for males (11% and 4.5% respectively) (Lawrence et al. 2015).
Over half (56%) of young people aged 13–17 who had self-harmed in the past 12 months had used services for emotional or behavioural problems. The proportion of females (61%) was higher than that for males (40%) (Lawrence et al. 2015).
Self-harm and mental disorders
In 2013–14 among young people aged 12–17:
- the highest rates of self-harm in the 12 months prior to the survey were among those with major depressive disorders (47% based on self-report and 33% based on parent/carer report)
- the rate was lower (11%) for those with an ‘other’ disorder based on parent or carer report, but still more than twice as high as for those for whom no disorder was reported (4.2%) (Lawrence et al. 2015).
Box 3: How many hospitalisations are for self-harm?
Suicidal ideation or suicide attempts may result in admission to hospital for specialised mental health care. National admitted patient hospital data cannot be used to distinguish between non-suicidal intentional self-harm and suicide attempts, so activity relating to these types of presentations is collectively reported as intentional self-harm.
In 2018–19, among young people aged 15–24:
- there were 9,600 hospitalised cases for intentional self-harm – a rate of 297 per 100,000, and 13% of all hospitalised cases for injuries among this age group
- the rate for females was 2.7 times as high as that for males (437 compared with 164 per 100,000). For 15–19 year olds, the female rate was 3.5 times as high as that for males; for 20–24 year olds, the female rate was twice as high as that for males.
While data on 15–24 year olds are presented here, self-harm can start at younger ages. In 2017–18, there were 1,100 hospital separations for intentional self‑harm for children aged 10–14 – a rate of 76 per 100,000 children. The rate for girls was 7 times as high as that for boys (136 and 19 per 100,000, respectively) (AIHW: Pointer SC 2021).
Due to a break in series in 2017–18, time-series analysis is presented only for 2007–08 to 2016–17 (see Technical notes for more details).
Between 2007–08 and 2016–17:
- cases of self-harm increased from 227 per 100,000 in 2007–08 to 344 per 100,000 in 2016–17
- the greatest increase was for females aged 15–19, which rose from 359 per 100,000 in 2007–08 to 686 per 100,000 in 2016–17 (Figure 4).
Figure 4: Hospitalised cases of self-harm for young people aged 15–24, 2007–08 to 2016–17
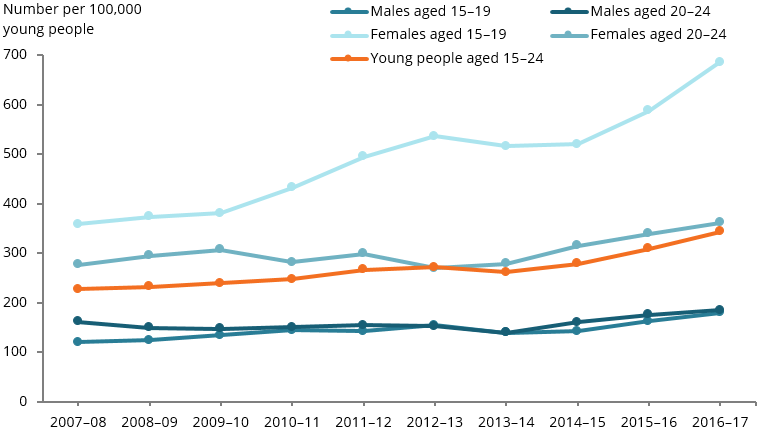
Chart: AIHW.
Source: AIHW NHMD.
In 2018–19, among young people aged 15-24, the rate of hospitalised cases for intentional self-harm varied across remoteness areas. It was highest in Remote areas (535 per 100,000), followed by Outer regional areas (479 per 100,000), Very remote areas (442 per 100,000) and Inner regional areas (369 per 100,000). It was lowest in Major cities (251 per 100,000).
In 2016–17, the rate of hospitalised cases for intentional self-harm was 1.4 times as high for young people living in the lowest socioeconomic areas as for those in the highest areas (394 and 276 per 100,000, respectively) (see Technical notes).
It should be noted that the complete extent of non-fatal suicidal and self-harming behaviours in the community is unknown in Australia. Although, data on hospitalisations due to intentional self-harm provide an indication of the incidence of these behaviours in the community, only data on those with serious physical or mental health issues admitted for further treatment are included (AIHW: Pointer 2021).
Information on hospitalisations for intentional self-harm reported here may differ from that in other publications. The differences are small and may reflect differences in the inclusion criteria (for example, Y87.0 is included here) and/or exclusion criteria. See also Technical notes for methodological issues.
How many deaths are due to suicide?
In 2019, based on ABS Causes of Death data, among young people aged 15–24:
- there were 461 deaths due to suicide, a rate of 14 per 100,000 young people
- the rate was much higher among males than females (20 and 7.6 per 100,000, respectively)
- for both males and females, the rate was higher among those aged 20–24 (24 and 8.5 per 100,000, respectively) than among those aged 15–19 (16 and 6.6 per 100,000, respectively).
Has there been a change over time?
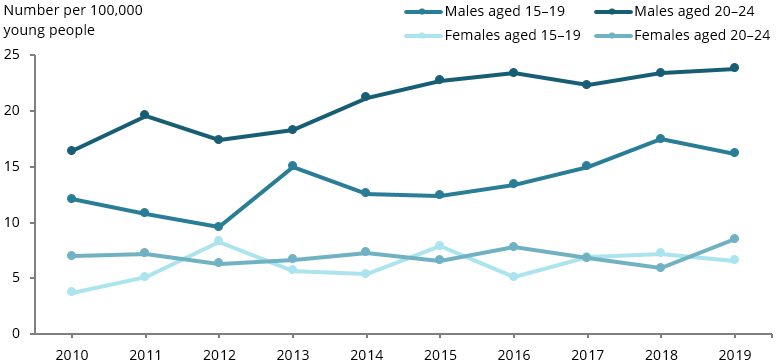
Between 2010 and 2019, based on ABS Causes of Death data, among young people aged 15–24:
- the rate of death by suicide increased from 10 per 100,000 young people to 14 per 100,000, with rates consistently higher for males than females (Figure 5)
- based on rate differences for 2010 and 2019, the largest percentage increases were for females aged 15–19 (from 3.7 to 6.6 per 100,000) and for males 20–24 (from 16 to 24 per 100,000) (Figure 5).
Caution should be exercised when analysing trends in deaths by suicide by young people (especially with regard to year-to-year changes) due to the small numbers of deaths by suicide each year. Deaths of young people attributed to suicide can also be influenced by reporting practices.
Figure 5: Deaths by suicide among young people aged 15–24, by age and sex, 2010–2019
Note: These data have been adjusted for Victorian additional death registrations in 2019. See Technical notes for more details.
Chart: AIHW.
Source: ABS Causes of Death, Australia, 2020.
Box 4: Ambulance attendances for suicidal behaviour and mental health
In 2019, based on the AIHW’s 2019 Quarterly Snapshot in selected jurisdictions (see Technical notes for details), ambulances attended the following incidents for young people aged 15–24:
- 5,300 incidents involving suicidal behaviours (suicidal ideation – 3,200; suicide attempt – 2,100)
- 1,200 incidents involving self-harm (without suicidal intent)
- 4,700 incidents involving mental health.
Due to the low number of ambulance attendances for deaths by suicide, these data cannot be reported by age and sex (AIHW 2020b).
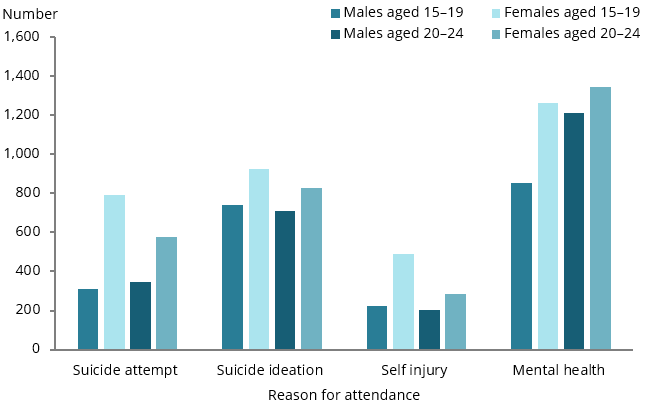
The number of incidents involving suicidal behaviours was higher among those aged 15–19 than among those aged 20–24. For both age groups, the number was consistently higher for females than males (Figure 6).
The number of incidents involving mental health was lower among those aged 15–19 than among those aged 20–24. For both age groups, the number was higher for females than males (Figure 6).
Figure 6: Number of ambulance attendances for self-harm behaviours and mental health in selected jurisdictions and months for young people aged 15–24, by age and sex, 2019
Note: National totals include data from New South Wales, Victoria, Tasmania and the Australian Capital Territory. Data were collected during March, June, September and December 2019 for ambulance attendances in Victoria, Tasmania and the Australian Capital Territory. Data for incidents in New South Wales were collected during June, September and December 2019.
Chart: AIHW.
Source: AIHW 2020b.
Are rates of mental illness the same for everyone?
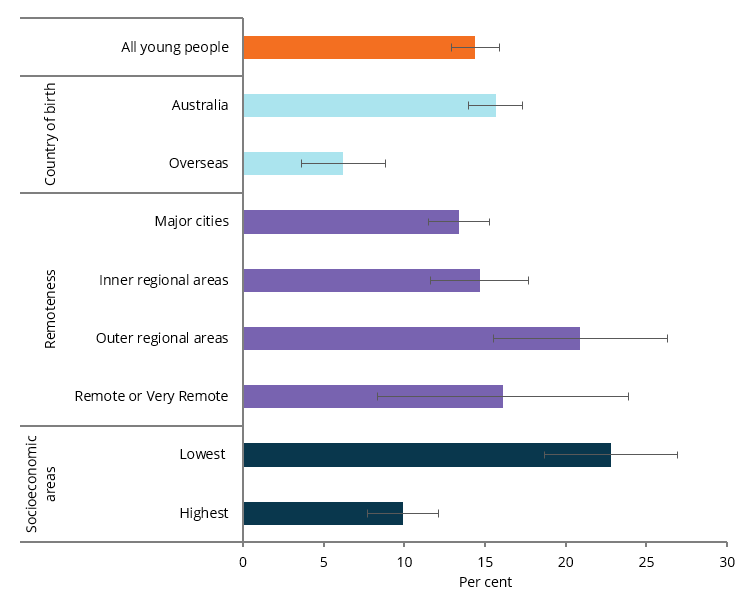
In 2013–14, based on the Young Minds Matter survey, the prevalence of mental health disorders among young people aged 12–17 was:
- 2.5 times as high among those born in Australia as among those born overseas (16% and 6.2%, respectively) (Figure 7).
- 1.6 times as high in Outer regional areas as in Major cities (21% and 13%, respectively)
- 2.3 times as high among young people living in areas of lowest socioeconomic status as among those living in areas of highest socioeconomic status (23% and 9.9%, respectively).
Figure 7: Mental illness among young people aged 12–17(a), by selected population groups, 2013–14
(a) In the 12 months before the survey.
Note: Data are based on parent and/or carer-report.
Chart: AIHW.
Source: AIHW analysis of the Young Minds Matter Survey Results Query Tool.
In 2017–18, based on the ABS National Health Survey, among young people aged 15–24, there was no statistically significant difference in the prevalence of mental or behavioural conditions across remoteness areas, or between the highest and lowest socioeconomic areas.
Where do I find more information?
For information on topics related to mental health in Australia’s young people, see:
For information on Indigenous young people and mental health, see:
- Indigenous young people and mental health: Section 7.5 of Aboriginal and Torres Strait Islander adolescent and youth health and wellbeing 2018
- Measure 1.18, Social & emotional wellbeing of the Aboriginal and Torres Strait Islander Health Performance Framework (HPF) report 2020
- mental health disorders: The Mental Health of Young people and Adolescents: Report on the second Australian Child and Adolescent Survey of Mental Health and Wellbeing and The Young Minds Matter Survey Results Query Tool
- mental health-care services and support, including presentations to EDs, hospitalisations and prescriptions related to mental health: Mental health services in Australia
- death by suicide and self-harm: AIHW’s Suicide and self-harm monitoring
- whole-of-population injury hospitalisations and deaths (including disaggregations for young people aged 15–24): Injury in Australia, 2017–18.