Medicare access
People in prison are currently ineligible to use Medicare and most Pharmaceutical Benefits Schemes. One reason for this is that Medicare and Pharmaceutical Benefit Schemes are federally funded, while prison clinics are funded and operated by the states and territories.
Having affordable, bulk-billed or subsidised health services and medications is necessary for the continuity of care of people leaving prison (Cumming et al. 2018; Kinner et al. 2012). So having access to Medicare services immediately on release is critical for the health of the person and the community. Prison dischargees were asked whether they would be enrolled in Medicare and able to access health services in the community on the first day of their release from prison.
Almost 9 in 10 (89%) prison dischargees reported they would be able to use Medicare services from the day of their release (Indicator 3.1.19).
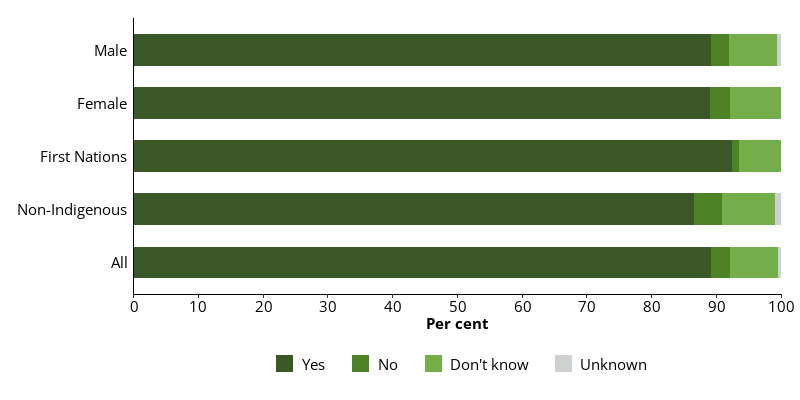
One in 10 dischargees were either unsure (7.4%) or reported they would not (2.8%) be able to use Medicare services from the day of their release (Figure 10.16).
Male and female prison dischargees (both 89%) were equally as likely to report they would be enrolled in, and have access to, Medicare services immediately on their release from prison (Figure 10.16).
First Nations prison dischargees (93%) were more likely than non-Indigenous dischargees (87%) to report they would be enrolled in, and have access to, Medicare services from the first day of release from prison (Figure 10.16).
Figure 10.16: Prison dischargees, self-reported access to Medicare on first day of release, by sex and Indigenous identity, 2022
Notes
- Proportions are representative of this data collection only, and not the entire prison population.
- Excludes Victoria, which did not provide data for this item.
Source: Dischargees form, 2022 NPHDC.